Is 8 pounds a big baby
Your Newborn's Growth (for Parents)
From your baby's first day, doctors will keep track of weight, length, and head size. Growth is a good indicator of general health. Babies who are growing well are generally healthy, while poor growth can be a sign of a problem.
How Big Are Newborns?
Newborns come in a range of healthy sizes. Most babies born between 37 and 40 weeks weigh somewhere between 5 pounds, 8 ounces (2,500 grams) and 8 pounds, 13 ounces (4,000 grams).
Newborns who are lighter or heavier than the average baby are usually fine. But they might get extra attention from the doctors and nurses after delivery to make sure there are no problems.
Different things can affect a baby's size at birth. The length of the pregnancy is important. Babies born around their due date or later tend to be larger than those born earlier.
Other factors include:
- Size of parents. Big and tall parents may have larger-than-average newborns; short and petite parents may have smaller-than-average newborns.
- Multiple births. If you have twins, triplets, or more, you can count on your babies being a bit small. Multiples have to share their growing space in the uterus, and they're often born early, which leads to small size at birth.
- Birth order. First babies are sometimes smaller than brothers or sisters born later.
- Gender. Girls tend to be smaller, boys larger, but the differences are slight at birth.
- Mom's health during pregnancy. Things that can lead to a lower birth weight include a mother with high blood pressure or heart problems; or one who used cigarettes, alcohol, or illegal drugs during the pregnancy. If the mother has diabetes or is obese, the baby may have a higher birth weight.
- Nutrition during pregnancy. Good nutrition is vital for a baby's growth — before and after birth. A poor diet during pregnancy can affect how much a newborn weighs and how the infant grows.
 Gaining a lot of weight can make a baby more likely to be born bigger than average.
Gaining a lot of weight can make a baby more likely to be born bigger than average. - Baby's health. Medical problems, including some birth defects and some infections during the pregnancy, can affect a child's birth weight and later growth.
p
What About Preemies?
Premature babies generally are smaller and weigh less than other newborns. A preemie's weight will largely depend on how early he or she was born. The time an infant missed being in the womb was growing time, so the baby has to do that growing after birth.
Many pre-term babies are classified as having "low birth weight" or "very low birth weight." In medical terms:
- Low birth weight means a baby weighs less than 5 pounds, 8 ounces (2,500 grams) at birth. That's the case for about 1 in every 12 babies in the United States, so it's quite common.
- Very low birth weight means a baby weighs less than 3 pounds, 5 ounces (1,500 grams).

Most babies with low birth weight or very low birth weight were born prematurely.
Premature babies get special medical attention right away after they're born. A specialist called a neonatologist may help care for them. Many preemies spend time in the neonatal intensive care unit (NICU) while they get medical care.
Is Bigger Better?
A baby with chubby cheeks and dimpled thighs once was many people's picture of a healthy newborn. But a baby born much larger than average may have special medical problems that need attention.
Some very large babies — especially those born to mothers with diabetes, including gestational diabetes — may have problems for a few days keeping blood sugar levels up. They might need extra feedings or even IV (given into a vein)
glucoseto keep those levels from falling too low.
Will My Baby Lose Weight?
Yes, at first. Babies are born with some extra fluid, so it's normal for them to drop a few ounces when they lose that fluid in the first few days of life. A healthy newborn is expected to lose 7% to 10% of the birth weight, but should regain that weight within the first 2 weeks or so after birth.
A healthy newborn is expected to lose 7% to 10% of the birth weight, but should regain that weight within the first 2 weeks or so after birth.
During their first month, most newborns gain weight at a rate of about 1 ounce (30 grams) per day. They generally grow in height about 1 to 1½ inches (2.54 to 3.81 centimeters) during the first month. Many newborns go through a period of rapid growth when they are 7 to 10 days old and again at 3 and 6 weeks.
p
Should I Be Concerned?
Newborns are so small, and it can be hard to know if your baby is gaining weight the way he or she should. You may worry that your baby has lost too much weight in the first few days or isn't taking enough breast milk or formula. If so, talk to your doctor, who may ask you about:
- How many feedings a day your baby gets. A breastfed baby may feed about 8 or more times in a 24-hour period; formula-fed babies usually eat less often, perhaps every 3 to 4 hours. A lactation (breastfeeding) counselor can make suggestions to increase comfort and improve technique, if a mom needs extra help.

- How much your baby eats at each feeding. A baby generally nurses for at least 10 minutes, should be heard to swallow after 3 or 4 sucks, and should seem satisfied when done. At this age, formula-fed babies may drink up to 3 to 4 ounces (90 to 120 milliliters) at a time.
- How often your baby pees. A breastfed baby may have only 1 or 2 wet diapers a day until the mother's milk comes in. Expect about 6 wet diapers by 3 to 5 days of age for all babies. After that, babies should have at least 6 to 8 wet diapers a day.
- How many bowel movements your baby has each day, and what they're like. Newborns may have only one poopy diaper a day at first. Poop is dark and tarry the first few days, then becomes soft or loose and greenish-yellow by about 3 to 4 days. Newborns usually have several poopy diapers a day if breastfed and fewer if formula-fed.
What Else Should I Know?
Being small or large at birth doesn't mean a baby will be small or large later in childhood or as an adult. Plenty of tall teens began life as small babies, and the biggest baby in the family can grow up to be a petite adult.
Plenty of tall teens began life as small babies, and the biggest baby in the family can grow up to be a petite adult.
By the time they're adults, kids tend to resemble their parents in size. Genetics, as well as good nutrition and your attention, will play a large part in how your baby grows in the years to come.
Whether your baby starts out large, small, or average, in the next few months you can expect your little one to keep growing fast.
Reviewed by: Madhu Desiraju, MD
Date reviewed: October 2018
Worried about having a big baby? Four things to know about birth weight | Your Pregnancy Matters
As my patients approach their final weeks of pregnancy, they typically start asking questions about how much the baby will weigh and what that means for delivery.
Doctors think about this too. We try to accurately determine the weight of the unborn baby so we can make the best possible birth plan. But predicting birth weight is actually very difficult to do.
In a recent study, one-third of women reported their OB provider told them their baby might be getting “quite large” near the end of pregnancy. In the end, however, only one in five of those women had a baby that weighed more than 8 pounds, 13 ounces or 4000 grams, a common threshold for labeling a baby “large.”
It would be nice to know the exact birth weight of a baby before it’s born – it makes predicting some rare, but serious complications like birth trauma easier. But that’s just not possible, and our estimates of your baby’s size can potentially cause unnecessary stress on mom and lead doctors to intervene when nothing is really necessary.
Here are some things to think about as you approach the end of pregnancy and are wondering what your baby might weigh and how this could impact your labor and delivery experience:
1. What is considered a ‘big baby’?
Picking an absolute cut-off is tricky. Typically, we consider estimated weights of babies that weigh more than 4500 grams (10 lbs. ) as larger than normal (or “macrosomic”). But what we really want to know is whether your baby is too big for your pelvis.
) as larger than normal (or “macrosomic”). But what we really want to know is whether your baby is too big for your pelvis.
Weight is just one factor doctors consider when we’re estimating the chances of a patient successfully having a vaginal delivery. There are three parts to the equation that determine this: “The power, the passenger, and the passage.”
The “power,” or force of uterine contractions, is something we can only assess when labor begins.
The “passenger” refers to the baby. His or her weight isn’t the only factor – the exact position of the baby within the birth canal also plays an important part in making it out successfully. The direction the head is facing can make all the difference in how easily the baby descends in the birth canal.
“Passage” refers to the anatomy of your pelvis. When doctors do vaginal exams toward the end of the pregnancy, that’s what we’re trying to evaluate: How narrow is the pelvis? Can we reach the tailbone? Do we think this baby will fit through this pelvis?
Like the estimation of fetal size, this isn’t an exact science, but it can help us determine a birth plan for the day of delivery.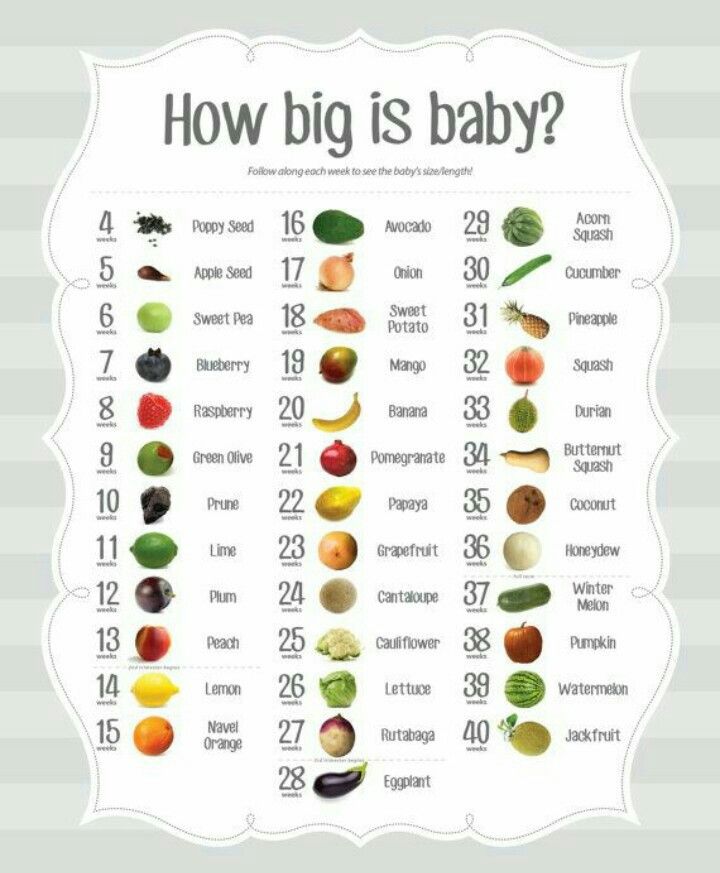
2. Ultrasound is not very reliable for estimating fetal weight near term.
For a 9-pound baby, an ultrasound’s predictive accuracy is typically 15 to 20 percent off. Which means we may over- or underestimate by more than a pound. Why is there such a wide range?
Ultrasound uses volumes to calculate fetal weight. It takes measurements of the head, waist circumference and some bones and comes up with an estimate. But it can’t measure the density of the fetal tissues directly.
I explain it to my patients like this: I can measure something with ultrasound the size of a brick. That structure will look the same whether made of Styrofoam or stone – but something made of stone obviously weighs a lot more than something made of Styrofoam.
There is a formula for calculating fetal weight based on standard measurements – but not all babies follow the rules for getting the weight accurate! There is no way to know exactly how much a baby is going to weigh until after the baby is born.
3. Who is really at risk for having a big baby?
Certain health and history factors put mothers at increased risk for having a large baby:
- Diabetes, including gestational diabetes, is a concern, especially if the mom’s sugar levels have not been controlled well during pregnancy. High glucose levels in mom can cross the placenta and lead to high levels in the fetus. As a response to these high sugar levels, the fetus produces insulin, which stimulates its own growth.
- Maternal obesity is another big risk factor. The rate of macrosomia has increased over time with rising obesity rates, so we expect to actually see more macrosomic babies in the future.
- History of a previous big baby. The trend is for successive babies to get bigger, not smaller, so this is something we would take into consideration.
If you are not in one of these categories and your health care provider has expressed concern about the size of your baby, I recommend having an honest conversation with him or her about their worries and recommendations.
4. What are the concerns about having a large baby?
We have to consider the possible risks to two patients – both mother and infant. The most serious risk of fetal macrosomia is birth trauma for the baby, especially something called a shoulder dystocia, where after the baby’s head is delivered the rest of his or her body does not deliver easily.
I’ve been in this situation before – it can be pretty frightening, and I completely understand why doctors are quick to recommend a C-section when worried about the possibility for a large baby – it’s an easier way to get the baby out safely.
At the same time, C-sections come with additional risk to the mom and result in additional hospital days, longer recovery periods and added costs. And since our estimates of fetal weight are frequently off, these risks may be unnecessary.
Making a plan that works for you
It is challenging to identify moms and babies that we really need to be concerned about. When doctors label a woman as having a possible “big baby,” we increase the possibility of using interventions during labor such as scheduled C-sections or labor inductions. The average weight of babies that were predicted to be “large” in the study I mentioned earlier was only 7 pounds, 11 ounces – not so big after all.
When doctors label a woman as having a possible “big baby,” we increase the possibility of using interventions during labor such as scheduled C-sections or labor inductions. The average weight of babies that were predicted to be “large” in the study I mentioned earlier was only 7 pounds, 11 ounces – not so big after all.
The recommendations from the American Congress of Obstetricians and Gynecologists are clear. ACOG says ultrasound is no better than a provider’s exam in estimating fetal weight, suspected macrosomia should not be an indication for induction of labor, and planned C-sections shouldn’t be performed unless the estimated fetal weight is 10 pounds or more in diabetic women or 11 pounds or more in other women.
I recommend having an open and frank discussion with your doctor about the clinical information available to you. Discuss the estimated size of your baby, your obstetrical history, your physical exam, and your risk factors. Balance the potential risks and benefits to both you and your baby when making your final decision.
For more information about pregnancy, labor, and delivery, sign up to receive Your Pregnancy Matters email alerts when we publish new stories. You can also make an appointment to see one of our specialists by calling 214-645-8300.
"We thought about having three children." How does a British family live in which
For 26 years of marriage, the British Noel and Sue Radford had 20 children. Their first child Chris was born when Sue was only 14 years old. Four years later, she and Noel got married. Now the oldest child of the Radfords is 29 years old, and the youngest is barely nine months old. We tell you how the largest family in the UK lives and how many liters of milk they drink a day.
Mother of many children from a foster family
In November 2018, Sue and Noel Radfort welcomed a baby girl named Bonnie. This was actively written in the British press and told on TV. That's because Bonnie is their 21st child. A year earlier, under the same scrutiny of the media, they took Archie, their 20th child, from the hospital.
Sue and Noel met when Sue was 7 and Noel was 12 years old. Both grew up in foster families - their parents abandoned them at birth. At 13, Sue became pregnant, at 14 she gave birth, but the young people decided not to send the child to an orphanage. They left him and stayed together. Sue and Noel got married as soon as she turned 18.
During their 26 years of marriage, the couple had 20 children; the last, Bonnie, Sue became pregnant at 42. Their eldest son, Chris, is 29, Sophie is 25, Chloe is 23, Jack is 22, Daniel is 20, Luke is 18, Millie is 17, Kathy is 16, James is 15, Ally is 13, Amy is 13. , Josh is 11, Max is 10, Tilly is 8, Oscar is 7, Casper is 6, Hallie is 3, Phoebe is 2, Archie is a year old, and Bonnie is 9 months old.
“At first we thought we'd stop at three, but we love having kids around so much that we can't stop. We are very used to children and love them,” says Noel. After the birth of his seventh child, he had a vasectomy, but then changed his mind and performed a reverse operation.
The couple lives with their 19 children in a 10-room house they bought in 2004 for £240,000. They run a blog where they talk about family holidays, weekdays, vacations, budget recipes, and even makeup secrets for girls.
So far, only the eldest daughter, Sophie, has started her family, and she also has many children: she has three children. Oscar, Sue and Noel's son, now seven, was born the same year as their first grandson. For now, Sophie is going to focus on three children: according to her, she could not do as much every day as her mother does for children.
In total, Sue Radford was pregnant for 811 weeks, that's 15.5 years.
Savings on movies and trampolines
The Radfords' main source of income is government-sponsored child support and the family bakery. Children help in it: Chloe bakes and comes up with new recipes for pies, Daniel helps to take orders and monitors delivery.
The smallest amount Sue Radford spends on groceries in one week is £310. In the summer, when most of the kids are on vacation, £435.
Every day the family drinks 10 liters of milk, three liters of juice, and eats three boxes of cereal for one breakfast. But the family rarely goes to them, not only because of the price: not every institution is ready to accommodate almost 20 people, even at lunchtime. Often you have to wait an hour until enough tables are free. “It's fun to look at the faces of the workers and other guests as the family of 20 sits down in a crowd,” says Sue.
Other entertainment is also expensive. If the average British family spends around £550 over the weekend, just going to the trampolines will cost the Radfords half that amount. Add to that a trip to the cinema and you have to throw another hundred pounds on top.
Family tickets, which are cheaper than regular tickets, are not suitable for them. As a rule, they are designed for two children and two adults. For the Radfords, this is clearly not enough. Sometimes they are rescued by discounts and promotional codes that they find on the Internet.
For the Radfords, this is clearly not enough. Sometimes they are rescued by discounts and promotional codes that they find on the Internet.
But the most memorable moments they spent with the whole family were walks in the park or picnics in nature, which cost almost nothing, Noel and Sue admit.
“There are many ways to go somewhere on a budget and have a good time. If I'm making a takeaway lunch for each of us, I need two loaves of bread, three packs of sausage rolls, 24 packs of chips. In bad weather, we stay at home, turn on the movies or play video games, sometimes we cook popcorn. Kids bully each other, of course—it’s normal for their age, especially since they all want different things,” says Sue.
18 kilos of laundry a day and clothes in a trash bag
Sue's day usually starts at 06:30 am and she doesn't go to bed until 11 pm. Now in British schools holidays, so the children spend most of the day at home. According to Sue, the house turns into a mess for a while, but nothing can be done - you just need to accept it.
“I prefer to clean up at the end of the day, after the kids have gone to bed. If you constantly clean a little bit during the day, it will take much more time. So I spend two to three hours daily cleaning,” says Sue. Every day she washes 18 kilograms of children's clothes - the machine has to be run three times a day.
But the most difficult thing with so many children is not to lose them on the journey. The family tries to go somewhere every year. This year they have already been to Florida, now they are going to the Netherlands. “You have to keep your eyes on the back of your head at all times. The older kids always help to keep an eye on the younger ones, so we've never lost anyone before, and the kids themselves never really hang out," says Sue. They usually travel in their 15-seater mini-bus.
Each trip, according to her, is like preparing for a military operation: “The hardest thing is to pack your bags. I put each child's clothes in a big trash bag and put a tag on whose clothes are in there. Then I just take out the right bag, focusing on the name, and not rummaging through all the contents. Especially since we usually take seven suitcases with us.”
Then I just take out the right bag, focusing on the name, and not rummaging through all the contents. Especially since we usually take seven suitcases with us.”
Hero parents or selfish parents?
The Radford family is considered the largest in the UK, so they are constantly riveted media attention. They even had their own reality show on the British Channel 4 TV channel. When the first season aired, only 16 children were mentioned in the title. The last issue, which was shown in January 2019, was already called "21 children, the report has gone."
But recently, British families, where the number of children is measured in double figures, often hear criticism addressed to them. In one of the television interviews, the 11-year-old daughter of the Radfords said that she experiences stress when she looks after her younger siblings. 19 live in the Radford housechildren, 15 of whom are under the age of 18. Parents have repeatedly said that older children help them look after the younger ones. In connection with this, the Radfords are accused of selfishness.
In connection with this, the Radfords are accused of selfishness.
In 2018, British blogger Fiona Foodhouse wrote in a private Facebook group that she lives “literally around the corner” from the Radfords and regularly sees their children with a nanny. In response, she began to write personal messages to Sue and her daughter. They denied the information that the family has a nanny. The Radfords accused Fiona of trying to promote their YouTube channel with this story, and Fiona accused them of harassment and blackmail.
Another issue is child benefits. Ordinary taxpayers believe that families with many children cost them too much. In the UK, more than seven million families receive cash assistance: £20.70 per week for the first child and £13.70 for each subsequent child. If a parent's income exceeds £50,000, they must pay tax on the allowance.
There are 305 British families with ten children and £2.3 million a year in benefits.
In 2015, the UK even offered to start paying child allowance only for the first three children. According to preliminary calculations, this would help save £300 million in the budget.
According to preliminary calculations, this would help save £300 million in the budget.
Read also
Where does the desire for excessive care for children come from
Why do the current generation of children have fewer friends in the neighborhood? Why has the culture of childhood and parental supervision changed so much in the last thirty years?
05/22/2017 3332 0
Rules for upbringing Ekaterina Burmistrova - Psychologist and Mom 11 (!) Children
“I would be scared to have one child”
04/04/2019 2829 0 9000 9000
Look at the Child, not the Libra http://www. Look at the Baby, Not the Scale translated by Veronika Savina Published with the permission of the author It sounds so simple, doesn't it? And yet I've seen so many babies who looked healthy, suckled well, but their moms lost confidence in breastfeeding because someone told them their baby's weight didn't match the charts. This Someone was looking at scales and charts, not at a child. Babies tend to lose approximately 3-10% of their initial weight in the first 24 to 72 hours after birth and then regain that weight over the next 2 to 3 weeks. If the mother received a lot of fluid during labor (intravenous fluids), the baby may be born "heavier" due to the increased water content. Babies who were weighed before they first urinated weigh slightly more. The difference from this fluid retention is a few ounces, but parents can be very concerned when their baby weighs a few ounces less than at birth when they check back two weeks later. Another common problem with early screenings is a child not gaining as much weight as is considered "normal". There is no general agreement on weight gain rates, and the range from various sources is 4 to 8 ounces (113 to 226g) per week. Some babies are genetically predisposed to be much smaller or larger than others. As I mentioned in the first paragraph: it's clear, isn't it? If you have been told that your child has not gained enough weight, look at this list of questions:
If you answered "Yes" to the above questions, you may be reminded of two important questions that "charts" usually ignore.
If someone asks you how much weight a 33 year old man should have, you will laugh. The range of weight possibilities varies depending on height, bone structure, ethnicity and many other factors. Babies, on the other hand, are expected to match their weight with a chart distributed throughout the country without assessing genetics, type of feeding, or any other factors. Most often, problems with attachment to the breast are the cause of slow weight gain; incorrect, ineffective nipple latch is probably the only common problem with breastfeeding in the first weeks. This, with the right help, is an easily fixable problem. Under favorable circumstances, breastfeeding should be assessed within the first day or two following days after birth by a qualified breastfeeding professional. Good hospitals have such specialists (LC and IBCLC's) on staff. If there are problems with attachment, the first answer should never be "supplementation", the best advice and help available should be found. Find qualified help, if possible, in person or by phone. There is nothing better than having an experienced lactation expert look after you and your baby and give you the help and support you need. A few notable examples: Child, birth weight: 9 lbs. 12 oz (4422 g). I have seen mothers who wanted to give supplements because "they don't have milk and the baby is hungry and losing weight." The baby looked good, was breastfeeding every 1 to 3 hours, and the mother's nipples were not sore. There was no need to do anything, just pick him up often, put him to the breast, shifting from one to the other every 5 minutes and so wait a day or two until the milk comes. A thirsty child often requires the breast and is safe. A baby who has been given water or formula will not breastfeed as much, and mom's confidence (and milk production) will suffer as a result. This mom only needs the support of an expert to make sure she knows how to breastfeed her baby. Same baby, two weeks check: 9 lbs. 6 oz (4252.5g) Forgetting that this 4 oz (113.4 g) weight gain from 36 hours after birth, some doctors might recommend supplementation. Again we observe breastfeeding and, if everything is fine, we do not worry. Same baby, six month check: 15 lbs. The breastfeeding consultation was successful in the first weeks thanks to the mother finding a good doctor and feeding her baby on demand. This big baby (9 lb 12 oz at birth, remember?) weighed 13 lb (5897 g) at four months and now weighs 15 lb (6804 g). The doctor notices and sees that mom is 5ft 3in (160cm) and dad is 5ft 9inches ( 175 cm ) and slender. He looks at the charts secondarily, at the baby first, and is not bothered by the drop in weight gain from a very high percentile* at birth to a lower one and then to an even lower one. I think that this is where I will end this story with a happy ending. In conclusion, babies who suckle frequently, pee light-colored urine, and have their diapers wet well in the first weeks of life are almost always fine. I can't think of a child in my experience for whom slow weight gain in the first 2 to 6 weeks was the ONLY sign of a problem. Older children, 2 to 12 months old, grow at varying rates. Weight gain should not be used as the main criterion for good health. Norms related to development and interaction with parents and others are more important. Do not supplement a baby who is doing well. Seek help with breastfeeding, and use health criteria other than weight for evaluation. Translator's Note: * The nth percentile is said to be the value below which n percent of observations of a given variable are located. Therefore, the 40th percentile (or 4th decile) is the value below which 40% of the observations fall; The 50th percentile is called the median, and the 25th and 75th percentiles are the lower and upper quartiles, respectively. Welcome
Find us on iTunes! |
 drjaygordon.com/bf/scales.htm
drjaygordon.com/bf/scales.htm 

 If there is no such specialist, please contact a consultant within the first 12 hours after delivery. Your pediatrician can help you with this. Otherwise, call La Leche League and ask the leaders who they can recommend in your area. This is an important step in becoming a parent and should not be missed.
If there is no such specialist, please contact a consultant within the first 12 hours after delivery. Your pediatrician can help you with this. Otherwise, call La Leche League and ask the leaders who they can recommend in your area. This is an important step in becoming a parent and should not be missed.  2 oz (4139 g).
2 oz (4139 g).  In various cases, if the baby's skin is dry, yellow in color, the urine is darker, the baby needs more help with feeding. This baby still should not be formula fed. Make sure the mother is drinking enough water, breastfeeding the baby often without a regimen (every 1 to 3 hours). Also note that she is getting help with attachment, especially if she has sore nipples.
In various cases, if the baby's skin is dry, yellow in color, the urine is darker, the baby needs more help with feeding. This baby still should not be formula fed. Make sure the mother is drinking enough water, breastfeeding the baby often without a regimen (every 1 to 3 hours). Also note that she is getting help with attachment, especially if she has sore nipples.