Infant brace for hip dysplasia
Pavlik Harness Treatment for Children
What is Pavlik harness treatment for children?
The Pavlik harness is a soft splint. It is most commonly used for treating infants with developmental dysplasia of the hip (DDH). It helps keep the infant's hips and knees bent and the thighs spread apart. It can also help promote healing in babies with broken thighbones (femurs).
DDH occurs when the hip joint does not form normally. The hip joint is a ball-and-socket joint. The socket is a cup-shaped structure in the pelvis called the acetabulum. The ball, or head, is the rounded upper end of the femur. In DDH, the cup-shaped cavity of the acetabulum is more shallow than normal. As a result, the head of the femur does not fit into it well. The femoral head may slide partially out of the socket (sublux). In severe DDH, the head of the femur can slide completely out of the socket (dislocate). It may stay dislocated.
Strong fibrous tissues called ligaments normally help hold the femoral head in the acetabulum. In DDH, the ligaments may become stretched and loose.
By holding your baby's legs out and bent, the Pavlik harness helps keep the femoral heads in their sockets. It allows the ligaments to tighten. It encourages normal development of the acetabulum.
Why might my child need a Pavlik harness treatment?
It is normal for the hips of infants to be a bit loose. But this usually resolves on its own. It is particularly common in babies who were born feet or bottom first (breech). If their hips are too loose, they can sublux or dislocate easily. They may need treatment.
If your healthcare provider has concerns about possible DDH, he or she may recommend that your baby go to an orthopedist for evaluation. Sometimes the evaluation can involve an ultrasound of the baby's hips. If your baby has DDH, the orthopedist will probably recommend a device such as a Pavlik harness to encourage your baby's hips to develop normally.
Girls and breech babies have the highest risk for DDH.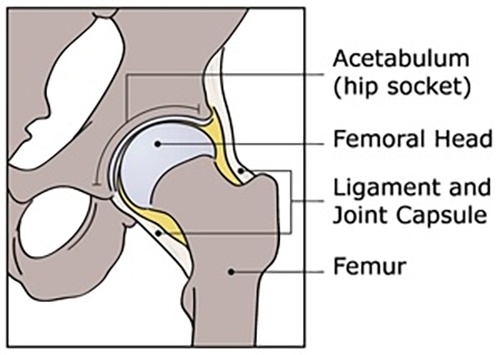 It also runs in some families. It is more common in first-born babies.
It also runs in some families. It is more common in first-born babies.
Healthcare providers sometimes use a Pavlik harness for femur fractures in infants younger than 6 months. The harness helps hold the baby's leg still so that the bone can heal.
What are the risks of Pavlik harness treatment for a child?
Pavlik harness treatment is usually successful in treating DDH. But sometimes complications can occur. They may include:
- Skin breakdown (dermatitis), especially in the groin, behind the knee, on the shoulder, or on the leg
- Lack of treatment success
- Nerve damage in the leg or shoulder
- Bone breakdown because of decreased blood supply (avascular necrosis)
- Flattening of the back of the femoral head
- Downward dislocation of the hip
- Subluxation of the knee
The most common complication is skin problems. You can reduce the risk for these skin problems by keeping all appointments and having the straps of the harness adjusted by the orthopedist as needed. Only the orthopedist should adjust the straps. You should keep your baby’s skin clean and dry. Don’t use lotions, ointments, or powders under the harness. If nerve problems develop, they typically go away on their own. If the Pavlik harness is not successful, your child may need a rigid brace instead.
You can reduce the risk for these skin problems by keeping all appointments and having the straps of the harness adjusted by the orthopedist as needed. Only the orthopedist should adjust the straps. You should keep your baby’s skin clean and dry. Don’t use lotions, ointments, or powders under the harness. If nerve problems develop, they typically go away on their own. If the Pavlik harness is not successful, your child may need a rigid brace instead.
How do I help my child get ready for Pavlik harness treatment?
You should not need to do much to prepare for your child's Pavlik harness treatment. Your baby may need to wear the harness for several months. During this time, it will be important to keep your baby's skin clean and dry. That will include changing diapers often. Consider stocking up on leak-proof diapers. Also ask what type of clothes to bring when you take your baby in for the first fitting. Your baby will need regular follow-up visits for harness adjustments and monitoring as he or she continues to grow.
What happens during Pavlik harness treatment for a child?
The Pavlik harness is a soft splint with a number of straps that fasten. It consists of a chest strap and leg straps. The chest strap goes across the baby's back and reaches around to close in the front. The leg straps attach to the front of the body strap, loop under each foot, cross over in the back, and attach to the top of the body strap. Each leg strap has two additional straps that wrap around the lower leg. The harness helps support the baby's legs in a bent, outward-rotated position. It prevents the baby from straightening his or her legs. It makes it hard for the baby to bring his or her legs together.
At first you should keep your baby in the harness all the time. You will learn how to put on your baby's clothes without taking off the harness. You will also learn how to change your baby's diaper in the harness. You may need to give your baby sponge baths with the harness on instead of full baths with the harness temporarily off. You will need to make sure to dry your baby well after bathing and after diaper changes.
You will need to make sure to dry your baby well after bathing and after diaper changes.
The harness is adjustable, so it can change as your baby grows. You will need to visit your baby's orthopedist regularly for adjustments. It is very important to have your baby's legs positioned correctly. Only allow the healthcare provider to make the adjustments. Do not try to adjust the harness yourself.
Your baby will also need regular ultrasounds to follow development of the hip joint. If the harness does not seem to be working within about 3 weeks, your baby's orthopedist may recommend using a cast or having surgery instead.
The orthopedist will tell you when you can take your baby out of the harness. After about 6 weeks, you will be able to take your baby out of the harness during the day. The baby will need to continue wearing the harness at night for about 6 more weeks.
What happens after Pavlik harness treatment for a child?
Most children have normal hip development after Pavlik harness treatment. It is important to continue follow-up as recommended by your child's orthopedist. Follow any instructions your child's orthopedist gives you. If your child has problems walking or seems to be in pain, he or she may need more treatment. Your child may need follow-up exams and imaging tests such as ultrasound or X-ray. Talk with your child's orthopedist about other signs to watch for. Ask when you should bring your child in for evaluation.
It is important to continue follow-up as recommended by your child's orthopedist. Follow any instructions your child's orthopedist gives you. If your child has problems walking or seems to be in pain, he or she may need more treatment. Your child may need follow-up exams and imaging tests such as ultrasound or X-ray. Talk with your child's orthopedist about other signs to watch for. Ask when you should bring your child in for evaluation.
Next steps
Before you agree to the test or the procedure for your child make sure you know:
- The name of the test or procedure
- The reason your child is having the test or procedure
- What results to expect and what they mean
- The risks and benefits of the test or procedure
- When and where your child is to have the test or procedure
- Who will do the procedure and what that person’s qualifications are
- What would happen if your child did not have the test or procedure
- Any alternative tests or procedures to think about
- When and how will you get the results
- Who to call after the test or procedure if you have questions or your child has problems
- How much will you have to pay for the test or procedure
Pavlik Harness - International Hip Dysplasia Institute
Looking for Pavlik Harness Tips for Parents?
The Pavlik harness is specially designed to gently position your baby’s hips so they are aligned in the joint, and to keep the hip joint secure. It is typically used to treat babies from birth to six months of age.
It is typically used to treat babies from birth to six months of age.
Since it is almost impossible to secure one hip by itself in the harness, both hips need to be positioned in the harness even if there is a problem with only one hip. By positioning your baby’s hips in such a way that the hip joint is aligned and stable, it will help normal growth and development of the hip joint. There are several reasons why the harness needs to be used and the doctor will explain to you why it is necessary for your baby to be in one.
When starting treatment, most doctors recommend that the baby wear the harness or brace full-time for 6-12 weeks. Some doctors allow the Pavlik harness to be removed for bathing and diaper changes as long as the legs are kept apart to keep the hips pointed at the socket. Babies are checked every week or two to adjust the fit, check the progress, and screen for complications such as femoral nerve palsy. The doctor can adjust the straps as needed to fit your baby as he or she grows. Ultrasound or x-rays are also used to see how the hips are developing.
Ultrasound or x-rays are also used to see how the hips are developing.
Some orthopedic surgeons use the stress test to determine when it’s safe to discontinue the harness, others prefer to use the harness for a pre-determined amount of time because of concern that stress testing may prolong the period of time needed for the joint to become more stable. In cases where there is any doubt the Pavlik Harness can be discontinued and a fixed abduction brace may be substituted. There are some reports that this may speed the development of the hip better than continuing to use the Pavlik Harness.
If the treatment is working, after the hips become stable the harness or brace is worn part-time, usually at night, for another 4-6 weeks. Even after that, the baby may need to sleep in the harness or another brace for a few weeks as a safety measure.
These differences in treatment depend on physician preference and seem to lead to satisfactory results either way. The important thing is to determine whether the hip is located in the socket.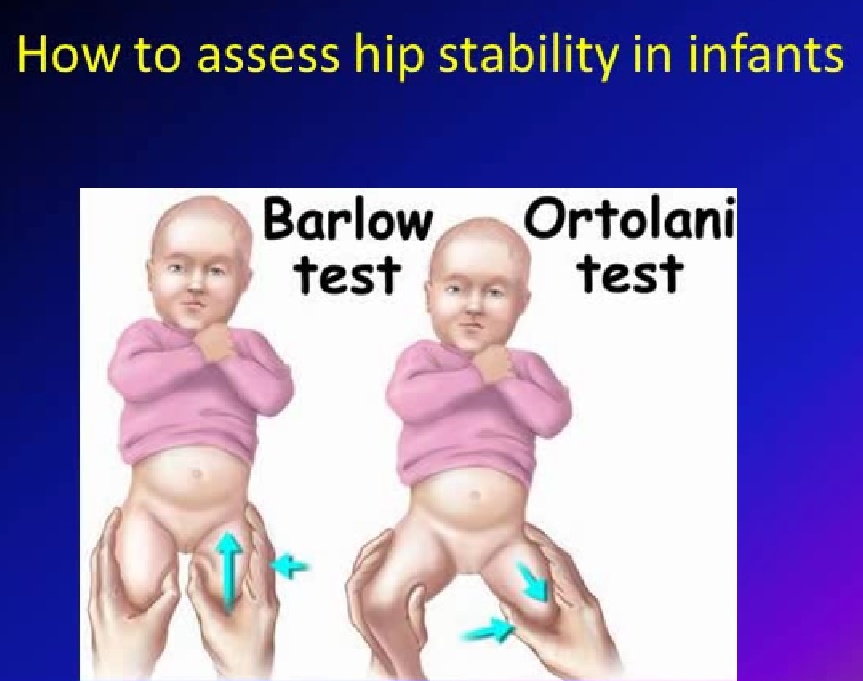 If the hip remains dislocated longer than 4-6 weeks, then the Pavlik harness needs to be stopped because continuing to use the Pavlik harness when the hip remains dislocated is very harmful to the hip.
If the hip remains dislocated longer than 4-6 weeks, then the Pavlik harness needs to be stopped because continuing to use the Pavlik harness when the hip remains dislocated is very harmful to the hip.
After appropriate and successful Pavlik harness treatment, there have not been any reported cases of re-dislocation. However, there is the risk of slow or incomplete development of the acetabulum (socket). This means that the hip will almost always stay in the socket, but the socket itself may become shallow or insufficient as the child grows. This is why x-rays are usually recommended for follow-up even when the harness has been successful. Once the x-ray is normal, then there’s probably a 99% chance that the hip will continue to grow normally. Recurrence of dysplasia is very rare after successful Pavlik harness treatment and a normal x-ray at 9-12 months old, but most doctors still recommend x-rays at an older age just to catch any shallow sockets that might need treatment to prevent early arthritis.
Founding Benefactors
3160 Southgate Commerce Blvd
Suite 50 Orlando, Florida 32806
Phone: (321) 843-5271 | Fax: (321) 843-5298 Copyright © 2023, International Hip Dysplasia Institute. All Rights Reserved. The content in this
website is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Website by Appleton Creative
Hip dysplasia - clinic "Family Doctor".
“Your child has hip dysplasia” - very often this phrase from the mouth of an orthopedic doctor causes a state close to emotional shock in the parents of the baby. But is everything so gloomy and scary, and what kind of pathology is this?
Dysplasia - this term means a violation of the formation of any organ or body system. In this material we will talk about hip dysplasia. nine0003
nine0003
Hip dysplasia is understood as a violation of the formation of the hip joint, which captures all the elements that make up the joint: the bone and cartilage base, the ligamentous-capsular apparatus and the muscle component. This definition is quite broad and includes the physiological immaturity of the hip joint, preluxation, subluxation and dislocation of the hip.
Physiological immaturity consists in the incomplete formation of the joint components without violating the congruence (correct matching) of the articular surfaces of the bones and, as a rule, requires minimal treatment or only dynamic observation, and it is this form of hip joint pathology that is mainly assigned the diagnosis of "dysplasia", although this is not entirely correct. terminologically. With pronounced immaturity of the hip joint, treatment is necessary to create favorable conditions for the proper maturation of the joint components. nine0003
Predislocation of the hip is already a pathology of the joint associated with the lack of stability of the femoral head in another component of the hip joint - the acetabulum and already requires close attention. In the absence of adequate treatment, hip predislocation can lead to the development of joint deformity (arthrosis), which leads to pain and impaired joint mobility, and can also lead to hip dislocation after the start of walking.
In the absence of adequate treatment, hip predislocation can lead to the development of joint deformity (arthrosis), which leads to pain and impaired joint mobility, and can also lead to hip dislocation after the start of walking.
Dislocation of the hip is the most severe form of the pathology of the development of the hip joint, which consists in the almost complete discrepancy between the articular surfaces of the femoral head and the acetabulum. Such a malformation of the joint requires maximum efforts for a thorough diagnosis and active and prompt treatment. Late diagnosis or inadequate treatment leads to gross impairment of the hip joint mobility and, ultimately, leads to disability. nine0003
Now we understand why so much attention is paid to hip dysplasia by pediatricians and orthopedists. Why is it the hip joint that is most susceptible to these misfortunes?
The fact is that the hip joint, due to its anatomical and physiological characteristics, is the most loaded joint in our body, and a failure in one of its constituent components leads to dysfunction of the joint and, ultimately, to a deterioration in the quality of life of the patient. That is why the diagnosis of hip dysplasia can so often be heard from the lips of an orthopedist, although one cannot but recognize the fact of some overdiagnosis of this pathology, but given the severity of the consequences in the absence of treatment, this is still justified. nine0003
That is why the diagnosis of hip dysplasia can so often be heard from the lips of an orthopedist, although one cannot but recognize the fact of some overdiagnosis of this pathology, but given the severity of the consequences in the absence of treatment, this is still justified. nine0003
According to statistics, the incidence of hip dysplasia is 4-6 cases per 1000 newborns, in girls it occurs 6-7 times more often. Unilateral lesion predominates over bilateral (more often the left hip joint is affected). There is inheritance from mother to daughter. Quite a lot of factors leading to impaired intrauterine joint formation have been noted, among them are breech presentation of the fetus, narrowness of the uterus, oligohydramnios, toxic and biological (primarily viral diseases of the mother during pregnancy) factors and much more. nine0003
When and by what methods can and should hip dysplasia be diagnosed? Can a mother herself suspect the presence of hip dysplasia in a child and, if so, with what methods? The answer to this question depends on the severity of the joint injury.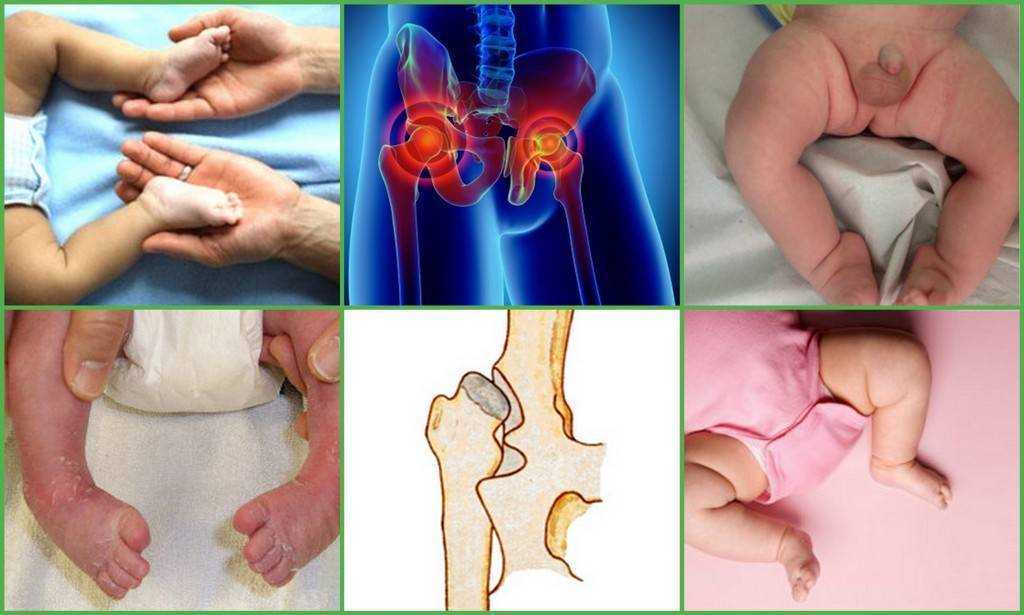 Let's try to answer this question by tying the timing and methods of diagnosis to the age of the baby.
Let's try to answer this question by tying the timing and methods of diagnosis to the age of the baby.
When conducting ultrasound diagnostics during pregnancy, it is possible to diagnose only gross violations - subluxation and dislocation of the hip, that is, those changes in which the articular surface of the femoral head does not correspond to the surface of the acetabulum of the child's pelvis. nine0003
In the first 7-10 days of a child's life, an examination can reveal a “click symptom” or “slipping symptom” - dislocation and reduction of the hip in the joint. These symptoms are revealed in a child as follows: in the supine position, the legs are bent at the knee and hip joints at an angle of 90 degrees. The thumbs are located on the inner surface of the child's thighs, the index and middle fingers on the outer. With careful abduction and traction of the hips, the femoral head is set into the acetabulum with a characteristic click. nine0003
After the 2nd - 3rd week of a child's life, limitation of hip abduction comes to the fore in the diagnosis of hip dysplasia. To identify it, the legs of the child bent at the knee and hip joints in the supine position are bred without violence. Normally, it is possible to spread the hips to an angle of 85-90 degrees to the surface. With increased muscle tone and spasm of the muscles adducting the thigh, abduction can be limited to an angle of about 70 degrees, but such a restriction of hip abduction can also be caused by impaired joint formation. Limitation of hip abduction on one side in most cases is a sign of pathology from the hip joint. nine0003
To identify it, the legs of the child bent at the knee and hip joints in the supine position are bred without violence. Normally, it is possible to spread the hips to an angle of 85-90 degrees to the surface. With increased muscle tone and spasm of the muscles adducting the thigh, abduction can be limited to an angle of about 70 degrees, but such a restriction of hip abduction can also be caused by impaired joint formation. Limitation of hip abduction on one side in most cases is a sign of pathology from the hip joint. nine0003
In favor of the pathology of the hip joint, symptoms such as shortening of one limb, turn of the foot on the side of the lesion outward from the middle position (external rotation of the foot) also speak.
The most widely known in parents (so to speak, "mommy symptom") - the asymmetry of the subgluteal folds - is not absolute and can be caused by many factors, but its importance in the diagnosis of hip dysplasia should not be underestimated, since this is the most common question that is addressed to orthopedic doctor. nine0003
nine0003
To confirm the diagnosis of hip dysplasia and control the dynamics of treatment, ultrasound diagnostics are currently widely used. The positive aspects of this method of examination include painlessness, non-invasiveness, relative safety and a sharp increase in recent availability. Also, with the help of an ultrasound examination of the joint, minimal changes in the structure of the hip joint can be detected. But, unfortunately, this examination method does not always give accurate results (its reliability is about 85-90%. Nevertheless, to date, ultrasound diagnostics is the main method of screening for the diagnosis of hip dysplasia.
In the case when the clinical picture differs from the data of the ultrasound examination or in case of late diagnosis of the pathology of the hip joint, the X-ray method is used. With a correctly performed radiograph, the picture of the structure of the joint and the position of the femoral head in the joint become completely clear. But due to the rather large radiation exposure during radiography, this examination method is used as rarely as possible. nine0003
But due to the rather large radiation exposure during radiography, this examination method is used as rarely as possible. nine0003
In children older than a year, the main symptom is lameness on the affected side when walking or a "duck" gait with a bilateral process. Diagnosis at this age is belated. The clinical picture in this case almost always requires confirmation by x-ray, since it is necessary to accurately determine the relative position of the joint components.
And so, the child was diagnosed with hip dysplasia, what to do next and how to help the baby? nine0003
Treatment of hip dysplasia should be started as early as possible. The goal of the treatment is to center the femoral head in the joint and create conditions for the formation of the entire acetabulum. Early, most gentle, but systematic treatment allows you to completely restore the anatomy and function of the underdeveloped hip joint.
The centering of the hip in the joint in the early stages of treatment is achieved by wide swaddling - two diapers are placed between the divorced hips of the child and fixed with a third. In severe degrees of hip dysplasia, special splints are used to center the femoral head (Pavlik's stirrups, Freik's pillow, etc.). When using these tires, parents may have questions and difficulties in caring for their baby, here are some tips to help you and your baby adjust during this period: nine0003
In severe degrees of hip dysplasia, special splints are used to center the femoral head (Pavlik's stirrups, Freik's pillow, etc.). When using these tires, parents may have questions and difficulties in caring for their baby, here are some tips to help you and your baby adjust during this period: nine0003
1. Only a baby diaper (disposable or gauze) should be under the stirrups or pillow. If you prefer to use gauze diapers, wear oilcloth panties that have zippers on the sides.
2. When changing a diaper, do not lift the child by the legs, but put your hand under the buttocks.
3. The vests can be changed without removing the stirrups: unfasten the shoulder straps from the chest strap and remove the vest over your head. nine0003
Over the tires you can wear loose pants, suits, dresses.
4. During the splint period, bathing the child is less frequent, so it is necessary to examine the skin under the straps, under the knees and around the neck 2-3 times a day to make sure there are no signs of inflammation (redness) of the skin.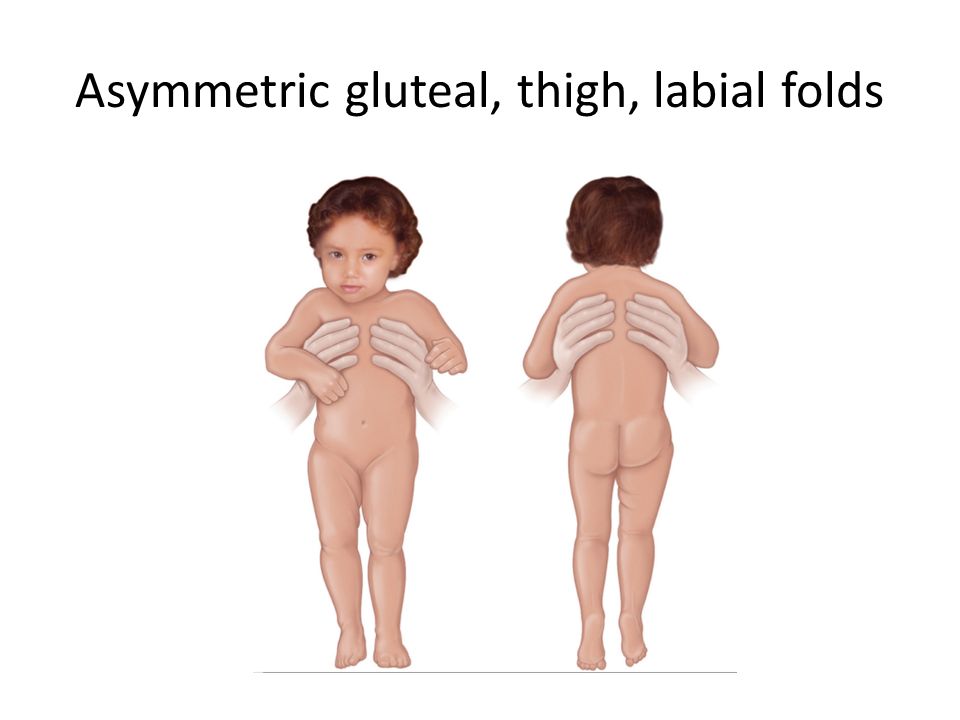 During this period, it is necessary to wipe the baby's skin with a soft cloth soaked in warm water. When carrying out water procedures, you can unfasten one foot part of the stirrup, but do not remove it, and keep the leg in a bent and retracted position. nine0003
During this period, it is necessary to wipe the baby's skin with a soft cloth soaked in warm water. When carrying out water procedures, you can unfasten one foot part of the stirrup, but do not remove it, and keep the leg in a bent and retracted position. nine0003
5. It is also necessary to monitor the hygienic condition of the tire itself, it must always remain dry, avoid getting powders and lotions under the belts, this can cause inflammation on the baby's skin.
6. When feeding, be especially careful to ensure that the baby's hips do not come together.
The wearing of these devices (orthoses) is long-term - from 3 months to a year, and it is extremely important for the parents of a child who has been diagnosed with hip dysplasia to be patient and not be cowardly during the treatment period and meticulously follow the doctor's prescriptions. nine0003
After centering the femoral head, they begin massage and therapeutic exercises aimed at creating the correct ratio of the articular surfaces. We can recommend some exercises that are easy to do at home.
We can recommend some exercises that are easy to do at home.
1. In the position of the child lying on his back, we bend the child's legs at the knee and hip joints as much as possible, and then fully straighten them.
2. In the previous starting position, we bend the child's legs at the knee and hip joints at a right angle, moderately spread the hips and, giving a moderate load along the axis of the hips, perform rotational movements with the hips. nine0003
3. In the position of the child lying on his back, we breed the legs of the child bent at the knee and hip joints as much as possible to the surface of the table.
All exercises are performed 8-10 times 3-4 times a day.
Also during this period, physiotherapy (paraffin baths, electrophoresis with calcium and phosphorus preparations) is used to improve the nutrition of the joint components and complex orthopedic massage.
In cases of late diagnosis of hip dysplasia or in the absence of adequate treatment in the early stages, treatment is carried out by long-term staged plastering, as well as surgical treatment, but in these cases there are no standard treatment regimens and patient care tactics are developed individually. nine0003
nine0003
After treatment of hip dysplasia, the child should be kept in the dispensary with an orthopedist for a long time - from 3 to 5 years until the end of growth. If necessary, control radiographs are performed once every 2 years to monitor the correct development of the joint. Also, restrictions on the load on the joint are often imposed. For children treated for hip dysplasia, it is desirable to visit specialized orthopedic groups in preschool institutions. nine0003
In severe degrees of hip dysplasia, functional disorders are, as a rule, lifelong in nature, even with timely and properly conducted treatment.
So what do the parents of the baby need to do in order to recognize hip dysplasia in time and, if this diagnosis was made to the child, to prevent serious complications?
First of all, it is necessary to show the child to the orthopedist in time. nine0015 The recommended terms of examination by an orthopedist are 1 month, 3 months, 6 months and 1 year.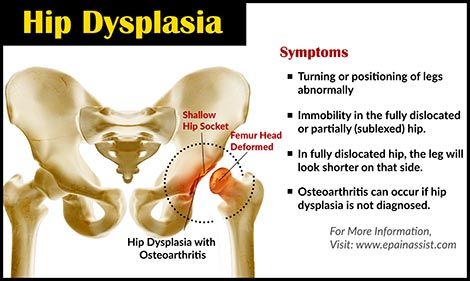
If the orthopedist nevertheless made a diagnosis of hip dysplasia, then the effectiveness of treatment by 50 percent depends on the correct and timely fulfillment by the child's parents of the doctor's prescriptions. It is important to remember that the sooner treatment is started, the better the results and the less chance of severe complications. With early diagnosis of hip dysplasia and correct and timely treatment, a positive result is achieved in 96-98% of cases. You should not be AFRAID of this diagnosis, but it is necessary to treat the child, he needs your help and care!
I hope this material helped you understand what kind of incomprehensible and frightening diagnosis it is - hip dysplasia, and it became clear to you how to deal with this pathology.
We recommend that you seek advice from the orthopedists of the Family Doctor clinic by calling the contact center in Moscow +7 (495) 775 75 66, or through the online appointment form. nine0003
Use of hip orthoses for dysplasia
Hip dysplasia of varying degrees is diagnosed in every 3-4 newborns. One of the conditions for successful therapy of pathology is the use of a children's bandage for the hip joints for several months.
One of the conditions for successful therapy of pathology is the use of a children's bandage for the hip joints for several months.
The effect of the use of children's cuts for the hip joint
Dysplasia in newborns refers to the immaturity of the main structures of the hip joint, which in the later life of the child can cause dislocations, clubfoot, flat feet and lameness. The treatment of pathology is complex, in addition to gymnastics, physiotherapy, drug therapy and massage, doctors recommend using special orthoses. The main task of such bandages is forced abduction and fixation of the hips at an angle of 90 or more degrees.
It is necessary to wear an orthopedic product for dysplasia for at least 6 months. During this time, the acetabulum assumes a normal shape and position, due to which the hip joint is stabilized.
Hip braces are effective for:
- Mild dysplasia.
- Congenital subluxation and preluxation of the joint.
Orthoses are also used to prevent dysplasia in children with a predisposition to joint instability. nine0003
nine0003
Bandages should not be used if the child already has a joint dislocation. They are temporarily postponed if there are damage to the skin or signs of dermatitis in the attachment area.
The duration of the use of children's hip orthoses is determined by the doctor based on diagnostic data. On average, therapy takes from 1 to 9 months, in severe cases, the child may need forced hip abduction up to one and a half to two years. A bandage for children with dysplasia must be purchased as early as possible, in this case, the joint recovers faster due to the immaturity of the tissues in the correct position. nine0003
Types of hip braces
The design of orthoses has some differences, some models are only suitable for correcting a pathology of a minor degree, others can also be used in cases where there is already a dislocation.
The most popular types of bandages for the hip joint are:
- Vilensky splint. It consists of two straps fixed on the ankles of the baby, and a metal spacer between them.
 This is the simplest orthosis in design; it is put on under the supervision of an orthopedist. The Vilensky tire must be worn constantly, removing only for the time of bathing. The band is available in three versions. The small size is suitable for correcting dysplasia for children up to three months old, the medium one can be worn up to a year, and the large one after a year; nine0107
This is the simplest orthosis in design; it is put on under the supervision of an orthopedist. The Vilensky tire must be worn constantly, removing only for the time of bathing. The band is available in three versions. The small size is suitable for correcting dysplasia for children up to three months old, the medium one can be worn up to a year, and the large one after a year; nine0107 - Frejka tire . Otherwise known as Frejka's pillow or duvet. It is a soft roller, fixed with straps on the shoulders of the baby. It is considered the most convenient and safe bandage, it can be used up to a year;
- Tubinger brace. Consists of a saddle with shoulder construction. It is possible to increase the spread of the legs and the length of the orthosis, so this bandage can be adjusted to the size of a growing child;
- Pavlik stirrups. Made from soft materials. It consists of bandages for the shin and chest area, shoulder straps and bending and retracting strips.
 Due to the stirrups, Pavlik's stirrups allow you to simultaneously move the legs to the sides and fix them in the desired position in the knees; nine0107
Due to the stirrups, Pavlik's stirrups allow you to simultaneously move the legs to the sides and fix them in the desired position in the knees; nine0107 - Tire Volkova. Rigid orthosis, includes tight bandages for the abdomen and back, and side parts for the legs. The tire fixes the limbs as tightly as possible. The product does not provide for changing the degree of fixation, so this orthosis is not very popular.
- Gniewkowski apparatus. The abductor splint is a modern, highly effective and convenient means of treating congenital diseases of the hip joint. The design of the diverting bar-spacer allows the use of one size for up to six months due to the ability to adjust the volume of the lumbar pad. In the same way, the size is selected for ages from 6 months to a year. nine0107
The appliances used need to be changed as the child grows, only this approach ensures the desired stabilization of the joint and the absence of complications during corrective therapy.
Features of choosing an orthosis
Trives hip brace (Frejk pillow) is a high-quality medical product.