How to make labor progress
Tips for Labor Progress - Spinning Babies
If labor is progressing on its own, don’t try and make it progress more. It is distracting and leads you away from your natural process.
If, on the other hand, labor is not progressing well on its own, and one of the following is occurring:
- Labor seems to start and stop, or just doesn’t pick up at all
- Labor pauses unexpectedly in the middle
- Contractions are strong without bringing any dilation
You may greatly benefit from some of the following suggestions.
Pre-Labor
(Contractions are irregular and last roughly 20-40 seconds, but are inconsistent.)When the baby isn’t fitting well, these contractions can be 60-120 seconds with no dilation. One sign can be that the labor pattern is erratic, but just don’t make an assumption. It can be difficult to tell this situation from a transition without a vaginal exam. See Comparing OA and OP Labor Patterns for more details.
In this phase, the following things can really help:
- Relax the abdomen with Rebozo sifting.
- Sit smart, with your back straight or a little forward to help the baby settle in the front of your abdomen.
- Abdominal and sacral releases
- Acupressure and acupuncture
- Chiropractic adjustment
- Warm chamomile tea
- Plenty of laughter and love!
Try and go about your day as normally as you can. Take a nap (but don’t forget to Rest Smart).
Is your abdominal wall loose? Does your uterus hang forward and make a crease underneath at the front of your panty line? Then use a pregnancy belt or a Rebozo to lift your uterus and allow the baby to come down on your cervix. Wear it until the baby is out to prevent a stall in labor after the head is born. Check-in with your provider(s) if any special needs present themselves.
Wear it until the baby is out to prevent a stall in labor after the head is born. Check-in with your provider(s) if any special needs present themselves.
Early Labor
(Contractions are regular and last 20-45 seconds with a frequency of 4-10 minutes apart. Things may begin to get bloody at this stage, which is normal.)In this early stage, the following tips can help:
- Relax the abdomen with the same things listed above in Pre-Labor.
- Maintain your regular daily routine. (Take into special consideration if your water broke.)
- Eat every two hours and drink lots of water, electrolyte drinks, and/or a little grape juice or hibiscus tea (for example) every hour.
- Rest Smart when you’re tired.
- Get up and walk or slow dance.
 Get down on your hands and knees and “wash the floor.”
Get down on your hands and knees and “wash the floor.” - Use gravity to your advantage with the Abdominal Lift.
- Kneel over the back of a couch or hospital bed. Or, kneel on pillows and rest your arms in a comfy chair.
- Try some lively hula-hoop circles on the Birth Ball for 20 minutes.
- Stand and lean forward in the shower if sitting is too painful. Do some pelvic circles while standing.
- Check-in with your provider(s) to let them know your potential for labor. If you have a doula, call them! Doula-supported labors are statistically proven to be shorter than labors without one.
Active Labor I
(Beginning around 4 cm dilation. Contractions last 60-75 seconds with a frequency of 3-6 minutes apart. )
)In this phase, the following advice can help:
- You may want quiet, dark privacy.
- Continue to Rest Smart when tired and use the relaxation methods above. Massage between contractions as well.
- Do more Rebozo sifting for serious relaxation.
- Walking can help contractions continue to come.
- Be sure to eat!
- Do more circles on the birth ball.
- Continue to lunge for one-sided pain.
- Try an inversion of one type or another (your preference).
- Then, do the Trochanter Roll (Walcher’s Maneuver) if the baby isn’t in the brim before now.
Are you confined to bed?
Some providers persuade or direct all their moms to stay in bed during labor. Sometimes a woman’s health is such that she has to stay in bed.
If this is the case, try the following techniques to help:
- Keep rotating the pelvis.
- Lay on your left side with a pillow between your knees, or lift your right knee high up on a stack of pillows and shift your left hip back behind you so your belly aims into the mattress. Use pillows to support what needs support. Switch to your right side and try each of the different variations.
- If you can kneel and lean over a birthing ball or the raised head of the bed, do so for 30 minutes between sides. Change positions every 30 minutes.
- If your labor starts progressing rapidly, don’t worry too much about position changes for the purpose of labor progress.
 If labor doesn’t continue to progress, try to keep your back straight, not curled.
If labor doesn’t continue to progress, try to keep your back straight, not curled.
Active Labor II
(Beginning around 5 cm dilation. Contractions last 60-85 seconds with a frequency of 3-5 minutes apart.)If you can cope through 5 cm, you’re likely to have a natural birth! Continue to follow these tips:
- Relax your involuntary muscles as described before. Or, if you have a loose, pendulous womb, wear a pregnancy belt during your entire labor.
- Rest Smart℠ when tired.
- At any time during active labor (through the next three described phases), you can:
- 1.) Do a sacral release
- 2.) Do the inversion through three contractions
- 3.
 ) Do a pelvic floor release
) Do a pelvic floor release
- Afterward, you will probably want to sink in a full tub or take a warm shower to mentally relax after those three techniques, which can be rather challenging this far into labor, but amazingly effective.
- Abdominal lift and tuck as before to take advantage of gravity. Do this for 10 contractions in a row, resting in between.
- Lunge for 6 contractions on each side. I like to do 3 contractions on one side, then switch knees and repeat, rather than all 6 on one side.
- Stand and hang onto your partner’s neck, or onto a sheet thrown over the bathroom door. (Tie a knot in one end and throw the knot over the door, then shut the door with the knot on the other side. Now the sheet won’t slip off the door and you can hang on and bend your knees and move to the contractions.
 )
) - Lift one hip and put one foot up. For instance, when sitting on the toilet, put one foot on a stool (or anything of a similar height) for three contractions. Stand for one with your other foot up on something. Then sit for three, stand for one, and repeat.
- Slow dance or slow dance in the shower while your partner sprays your back with a warm stream of water from the shower hose.
Active Labor III
(Dilation has advanced to 6-8 cm. Contractions last 60-85 seconds with a frequency of 3-4 minutes apart.)If you’re not at your birth site yet, now is a good time to go! Once there, continue to follow these tips:
- Balance as before, then relax the throat by “cooing.” Deep, low tones are usually better than high-pitched ones.
- Lots of moms like to be low to the ground, as they feel grounded with their knees deeply bent.
 Try kneeling on the floor while leaning forward, for example.
Try kneeling on the floor while leaning forward, for example. - Need to speed things up? Sit on a toilet for three contractions, then stand for three, and then sit for three again.
- Birth balls are rarely desired this late in labor, but if you’re up for it, give it a try.
- Lunge if you haven’t before, or try again for three contractions on each side and repeat.
- Walking can still be helpful, but may not be practical.
- Put one foot up on something when standing. Have your knee out diagonally and a foot on a stool (or other item).
- You will know what you need as your body feels progress. If you feel lost or frustrated, return to a calm state and do a Side-lying Release on both sides, followed by shake the apple tree.

- Make the pelvis open on one side by putting one foot on a stool. (Or, anything else you happen to have handy!)
Active Labor IV
(Dilation increases to 8-10 cm. Contractions last 75-120 seconds with a frequency of 2.5-4 minutes apart. Likely to be plenty of blood present now.)In this stage, the following tips can help:
- Continue balancing as before. Inversions are a common success for the stall in posterior labor.
- Use of a doula or face-to-face support is commonly appreciated.
- Loud moaning to a rhythm and a cool cloth can also help.
- Stand and lean forward to utilize gravity.
- Continue to Rest Smart℠ when in bed.
- Stand and hang on to the Rebozo or give a squat bar a try through 3-6 contractions.
- Lunge, holding a Rebozo or a sheet and straightening the back. Bend your knees with contractions and move freely.
- Is the baby still too high? Try another Trochanter Roll with Walcher’s Maneuver.
- Follow that up with a side-lying pelvic floor release.
Pushing or Releasing
(The second stage has begun. Contractions are now 45-75 seconds long with a frequency of 3-5 minutes.)In this final stage, the following advice can help:
- Be upright, with your back long and extended—don’t curl your back! When labor is not progressing readily, let your back be straight the way it naturally wants to lengthen.

- Sit up on a toilet (the porcelain birthing stool), lay on your side with your back arched instinctually, or stand and lift your arms to hang onto something sturdy above you.
- Relax as best you can in between contractions. Let the contraction get started before pushing voluntarily. If you need to push, use exhale pushing to conserve your strength and mental stamina. At the end of each contraction, take several deep cleansing breaths. Smile and feel the joy.
- Make deep vocalizations, vowel sounds, or roaring as desired.
- Kiss your partner.
- Know that your baby is helping you by pressing that pain out of your body. Work as a team. Let the baby rock back and forth in your pelvis. This relaxes the tissues in the perineum.

- Use vertical positions or side-lying on the bed to open the pelvis.
- Do some “towel pull” squats for 3-6 contractions.
- Use a hot washcloth on the perineum, and a cold, wet washcloth on the anus to prevent or soothe hemorrhoids.
- Rock forward and back while kneeling and leaning over a birth ball or the raised head of the bed.
- Keep lunging if the baby is asynclitic.
8 Ways to Start Labor Naturally – Cleveland Clinic
You’ve been carrying a baby in your belly for 39 weeks, and the moment you’ve been waiting for is just around the corner. Oh, the anticipation!
And the uncertainty. And the exhaustion. And, frankly, the discomfort.
All of it can make those last few weeks or days or hours crawl by at a snail’s pace.
If you find yourself scouring pregnancy blogs and internet message boards for anything you can do to help nudge your body into labor, you’re definitely not alone. While there’s no guaranteed way to do it, there are some natural techniques that many women swear by.
Some of them are merely old wives’ tales, while others have actually been studied by researchers. But if you’re planning to try any method to jump start your labor, certified nurse midwife Jessica Costa, MSN, APRN, CNM advises that you discuss it first with your midwife or physician.
Here, she weighs in on which commonly used methods are safe to try, and which are worthy of caution.
WalkingThis is one of the simplest ways that women try to jump start their labor. No study has found it effective, but some have found that spending time upright during labor has the potential to shorten the process.
“Movement is not going to induce labor, but it can really help progress labor and get baby in a good position for birth,” Costa affirms.
The verdict: Do it – please! “I highly encourage women to stay active during their pregnancy and walk 30 minutes most days,” she says. “That helps with labor preparation, fetal positioning and endurance also.”
Sexual intercourseA few studies have found no difference in the timing of labor for women who have sex during the end of their pregnancy and those who don’t. But there’s a biological explanation that suggests it could be worth a try.
“Making love can help stimulate the body’s natural love hormone, oxytocin, and that’s what causes contractions,” Costa explains. “A woman’s orgasm can also help with contracting the uterus if the body is ready, and semen is a natural source of prostaglandins, which can soften the cervix.”
Advertising Policy
The verdict: Feel free to give it a try. If nothing else, it’s a good way to stay connected with your partner during this exciting and busy time.
PineapplePineapple is loaded with an enzyme called bromelain that is sometimes used to help get the bowels moving. It hasn’t been well researched, but the thought is that, since the uterus sits right next to the intestines, it might also become irritated and start to contract.
It hasn’t been well researched, but the thought is that, since the uterus sits right next to the intestines, it might also become irritated and start to contract.
The verdict: “If a woman is not in labor, it’s worth a shot,” Costa says. You’ll also get a nice dose of vitamin C, fiber and manganese.
Nipple stimulationStimulating the nipples releases oxytocin, and there is actually some solid research behind this method.
“Sometimes a mom comes in with her water broken but she’s not in labor, or labor has started and is slowing down,” Costa explains. “I will have her try nipple stimulation before we start Petocin (a drug that induces labor).”
The verdict: It can be effective. But she recommends that women do it only under supervision of a physician or midwife. It’s best to monitor the baby and make sure the baby is tolerating the stimulation.
Castor oilMade from the little-known castor bean, castor oil is a powerful laxative that stimulates the intestines. It may, in turn, irritate the uterus and cause contractions.
It may, in turn, irritate the uterus and cause contractions.
The verdict: It’s not for everyone, and it’s not without risks, so talk with your physician or midwife about whether it’s a good option for you.
“For some women it can work great, but for others it’s just going to cause a lot of diarrhea and a lot of trips to the bathroom,” Costa says. “Your body has to be ready for this to work, and your provider can help with the right timing. It can also cause dehydration, so staying hydrated is crucial if using this method.”
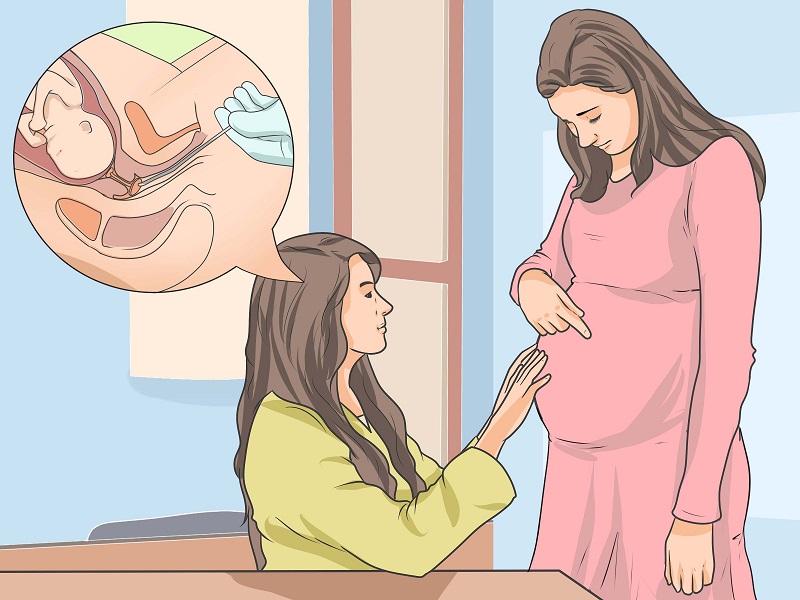
Membrane strippingThis procedure can be done during a visit with a physician or midwife once you’ve started dilating. They use a finger to separate the amniotic sac that surrounds the baby from the area around your cervix. This is thought to trigger the release of prostaglandins, which are hormones that soften the cervix and prepare the uterus to contract.
Advertising Policy
The verdict: Research is mixed on this one, and Costa says she counsels patients on an individual basis about this method.
“It isn’t without risks, like potentially breaking the bag of water, causing infection or irregular irritating contractions that don’t lead to labor,” she explains. “But for some women it can help lower their chances of needing a formal induction or shorten the length of pregnancy.” This is an option to discuss with your midwife or physician.
DatesAs in the fruit – not a candlelight dinner and a movie. Eating dates can help soften the cervix and promote spontaneous labor, Costa says. In one study, women who ate date fruit for four weeks prior to their due date were less likely to need a formal induction.
The verdict: Costa encourages all of her patients to eat six dates a day. Just make sure to buy the whole, pitted dates, rather than the ones that come diced up and covered in sugar.
Red raspberry leaf teaThis herbal tea rich in iron, calcium and vitamins won’t induce labor, but studies have shown that it’s safe and potentially beneficial during pregnancy.
“It’s a uterine tonic, so it won’t stimulate or shorten labor, but it can help spontaneous labor occur and make labor easier for women,” Costa says.
The verdict: She recommend women drink one to two cups a day starting at 32 weeks.
Perhaps the most important thing to do as you await the arrival of your new baby is the hardest to swallow – have patience.
“I tell people to enjoy the last days of the pregnancy as much as possible,” Costa says. “Sometimes you just need a tincture of time! I promise there will be an end.”
Induction of labor or induction of labor
The purpose of this informational material is to familiarize the patient with the induction of labor procedure and to provide information on how and why it is performed.
In most cases, labor begins between the 37th and 42nd weeks of pregnancy. Such births are called spontaneous. If drugs or medical devices are used before the onset of spontaneous labor, then the terms "stimulated" or "induced" labor are used in this case.
Labor should be induced when further pregnancy is for some reason unsafe for the mother or baby and it is not possible to wait for spontaneous labor to begin.
The purpose of stimulation is to start labor by stimulating uterine contractions.
When inducing labor, the patient must be in the hospital so that both mother and baby can be closely monitored.
Labor induction methods
The choice of labor induction method depends on the maturity of the cervix of the patient, which is assessed using the Bishop scale (when viewed through the vagina, the position of the cervix, the degree of its dilatation, consistency, length, and the position of the presenting part of the fetus in the pelvic area are assessed). Also important is the medical history (medical history) of the patient, for example, a past caesarean section or operations on the uterus.
The following methods are used to induce (stimulate) labor:
- Oral misoprostol is a drug that is a synthetic analogue of prostaglandins found in the body.
 It prepares the body for childbirth, under its action the cervix becomes softer and begins to open.
It prepares the body for childbirth, under its action the cervix becomes softer and begins to open. - Balloon Catheter - A small tube is placed in the cervix and the balloon attached to the end is filled with fluid to apply mechanical pressure to the cervix. When using this method, the cervix becomes softer and begins to open. The balloon catheter is kept inside until it spontaneously exits or until the next gynecological examination.
- Amniotomy or opening of the fetal bladder - in this case, during a gynecological examination, when the cervix has already dilated sufficiently, the fetal bladder is artificially opened. When the amniotic fluid breaks, spontaneous uterine contractions will begin, or intravenous medication may be used to stimulate them.
- Intravenously injected synthetic oxytocin - acts similarly to the hormone of the same name produced in the body. The drug is given by intravenous infusion when the cervix has already dilated (to support uterine contractions).
 The dose of the drug can be increased as needed to achieve regular uterine contractions.
The dose of the drug can be increased as needed to achieve regular uterine contractions.
When is it necessary to induce labor?
Labor induction is recommended when the benefits outweigh the risks.
Induction of labor may be indicated in the following cases:
- The patient has a comorbid condition complicating pregnancy (eg, high blood pressure, diabetes mellitus, preeclampsia, or some other condition).
- The duration of pregnancy is already exceeding the norm - the probability of intrauterine death of the fetus increases after the 42nd week of pregnancy.
- Fetal problems, eg, problems with fetal development, abnormal amount of amniotic fluid, changes in fetal condition, various fetal disorders.
- If the amniotic fluid has broken and uterine contractions have not started within the next 24 hours, there is an increased risk of inflammation in both the mother and the fetus. This indication does not apply in case of preterm labor, when preparation of the baby's lungs with a special medicine is necessary before delivery.

- Intrauterine fetal death.
What are the risks associated with labor induction?
Labor induction is not usually associated with significant complications.
Occasionally, after receiving misoprostol, a patient may develop fever, chills, vomiting, diarrhea, and too frequent uterine contractions (tachysystole). In case of too frequent contractions to relax the uterus, the patient is injected intravenously relaxing muscles uterus medicine. It is not safe to use misoprostol if you have had a previous caesarean section as there is a risk of rupture of the uterine scar.
The use of a balloon catheter increases the risk of inflammation inside the uterus.
When using oxytocin, the patient may rarely experience a decrease in blood pressure, tachycardia (rapid heartbeat), hyponatremia (lack of sodium in the blood), which may result in headache, loss of appetite, nausea, vomiting, abdominal pain, depression strength and sleepiness.
Induction of labor, compared with spontaneous labor, increases the risk of prolonged labor, the need for instrumentation
(use of vacuum or forceps), postpartum hemorrhage, uterine rupture, the onset of too frequent uterine contractions and the associated deterioration of the fetus, prolapse umbilical cord, as well as premature detachment of the placenta.
If induction of labor is not successful
The time frame for induction of labor varies from patient to patient, on average labor begins within 24-72 hours. Sometimes more than one method is required.
The methods used do not always work equally quickly and in the same way on different patients. If the cervix does not dilate as a result of induction of labor, your doctor will tell you about your next options (which may include inducing labor later, using a different method, or delivering by caesarean section).
ITK833
This informational material was approved by the Women's Clinic on 01/01/2022.
What will help in childbirth - articles from the specialists of the clinic "Mother and Child"
Vovk Lyudmila Anatolyevna
Reproductologist, Obstetrician-gynecologist
Lapino-1 Clinical Hospital "Mother and Child"
We walk and dance
If earlier in the maternity hospital, with the onset of labor, a woman was put to bed, now obstetricians, on the contrary, recommend that the expectant mother move . For example, you can just walk: the rhythm of steps soothes, and gravity helps the neck to open faster. You need to walk as fast as it is convenient, without sprinting up the stairs, it’s better to just “cut circles” along the corridor or ward, from time to time (during the aggravation of the fight) resting on something. The gait does not matter - you can roll over like a duck, rotate your hips, walk with your legs wide apart. It is worth trying and dancing, even if you think that you do not know how. For example, you can swing your hips back and forth, describe circles and figure eights with your fifth point, sway in a knee-elbow position. The main thing is to move smoothly and slowly, without sudden movements.
The main thing is to move smoothly and slowly, without sudden movements.
Showering and bathing
For many people, water is a great way to relieve fatigue and tension, and it also helps with painful contractions. You can just stand in the shower, or you can lie down in the bath. Warm water will warm the muscles of the back and abdomen, they will relax, and the birth canal will relax - as a result, the pain may decrease. Well, if it does not decrease, then in any case, the water will relieve stress and at least for a while distract from the pain. So if there is a shower or jacuzzi bath in the delivery room, do not be shy and try this method of pain relief for contractions. The only thing is that the water should not be too hot, even if it seems that heat helps to better endure contractions.
Swinging on the ball
Until recently, fitball (rubber inflatable ball) in the rodblock was something outlandish, and today is found in many maternity hospitals. And if you find a fitball in your rodblock, be sure to use it. You can sit on the ball astride and swing, rotate the pelvis, spring, roll from side to side. You can also kneel down, lean on the ball with your hands and chest and sway back and forth. All these movements on the ball will relax the muscles, increase the mobility of the pelvic bones, improve the opening of the neck, and reduce the pain of contractions. And while the woman is sitting on the ball, her partner (usually her husband) can massage her neck area for additional relaxation.
And if you find a fitball in your rodblock, be sure to use it. You can sit on the ball astride and swing, rotate the pelvis, spring, roll from side to side. You can also kneel down, lean on the ball with your hands and chest and sway back and forth. All these movements on the ball will relax the muscles, increase the mobility of the pelvic bones, improve the opening of the neck, and reduce the pain of contractions. And while the woman is sitting on the ball, her partner (usually her husband) can massage her neck area for additional relaxation.
To be more comfortable, the ball should be soft, slightly deflated, and large, with a diameter of at least 75 cm.
We hang on a rope or wall bar
When the contractions become very strong and painful, you can take poses in which the stomach is in a “suspended” state. Some advanced maternity hospitals have wall bars and ropes attached to the ceiling for this. During contraction, you can hang on them, as a result, the weight of the uterus will put less pressure on large blood vessels, and this will improve uteroplacental blood flow. In addition, in the “suspended” position, the load from the spine will be removed, which will also reduce pain.
In addition, in the “suspended” position, the load from the spine will be removed, which will also reduce pain.
Do not hang on a rope or a wall only if there is a desire to push, and the cervix has not yet opened and the efforts must be restrained.
Lying comfortably
If during childbirth a woman wants not to move, but, on the contrary, to lie down, then, of course, she can lie down. In modern maternity hospitals, instead of traditional ones, there are transforming beds: you can change their height, lower or raise the headboard or foot end, adjust the tilt level, push or push some part of the bed. There are also handrails in transforming beds (to use them to rest or even hang on them), and leg supports, and retractable pillows, and special backs - in general, everything in order to fit the bed under you and take it with it comfortable position. Moreover, this can be done without any physical effort - using the remote control.
We use everything we have
In any road block, even if it is minimally equipped, you can still find something useful. For example, if during a fight you want to take a position with a support, you can lean forward and rest against something that turns up under your arm - a table, a headboard, a window sill. The main thing is that the support must be very stable. You can also get on all fours in the “cat pose” and focus on your hands, and to make it more convenient, put a pillow and a folded blanket under your chest. If you want to hang on something (and there is no rope or wall) and your husband will be nearby, you can use postures that allow you to transfer body weight to him: for example, hang on your husband’s neck. In general, it is worth showing imagination and adapting any item in the rodblock to your needs.
For example, if during a fight you want to take a position with a support, you can lean forward and rest against something that turns up under your arm - a table, a headboard, a window sill. The main thing is that the support must be very stable. You can also get on all fours in the “cat pose” and focus on your hands, and to make it more convenient, put a pillow and a folded blanket under your chest. If you want to hang on something (and there is no rope or wall) and your husband will be nearby, you can use postures that allow you to transfer body weight to him: for example, hang on your husband’s neck. In general, it is worth showing imagination and adapting any item in the rodblock to your needs.
And don't be afraid to look stupid during childbirth. No one in the delivery room cares about how you move or lie down as long as it helps you get through your contractions, so calmly find your comfortable position.
Giving birth in an uncomfortable position is both difficult and inefficient.