How to have a big baby at birth
Having a large baby | Pregnancy Birth and Baby
beginning of content5-minute read
Listen
When you have a baby, one of the first things people like to know — besides the baby's name — is their birth weight. Even before the baby's born, parents can start to worry about its growth and development in the womb, particularly if they've been told they're having a big baby. But does size really matter?
Babies come in all shapes and sizes
More than 9 out of 10 babies born at term (37 to 40 weeks) weigh between 2.5kg and 4.5kg.
If your baby weighs 4.5kg or more at birth, they are considered larger than normal. This is also known as 'fetal macrosomia' and large for gestational age (LGA). (If they weigh less than 2.5kg, they may be considered smaller than normal. )
How is a baby's size measured?
During routine antenatal check-ups, your doctor or midwife may estimate the growth and size of your baby by measuring the 'fundal height'. That is the measurement from your pubic bone to the top of your uterus.
An ultrasound can also give health professionals an idea of how big your baby is likely to be, but it's not very accurate.
Your doctor may also check the level of amniotic fluid. Excessive amniotic fluid, which surrounds the baby in the womb, can indicate the baby is larger than average, since larger babies can produce more urine.
However, there's no way of reliably measuring your baby's weight until after they are born. In many cases, women who are told they're going to have a large baby actually give birth to a baby within the normal range.
Why is my baby big?
A baby may be large at birth due to genetic factors, the mother's health or, in rare cases, a medical condition that causes the fetus to grow too quickly.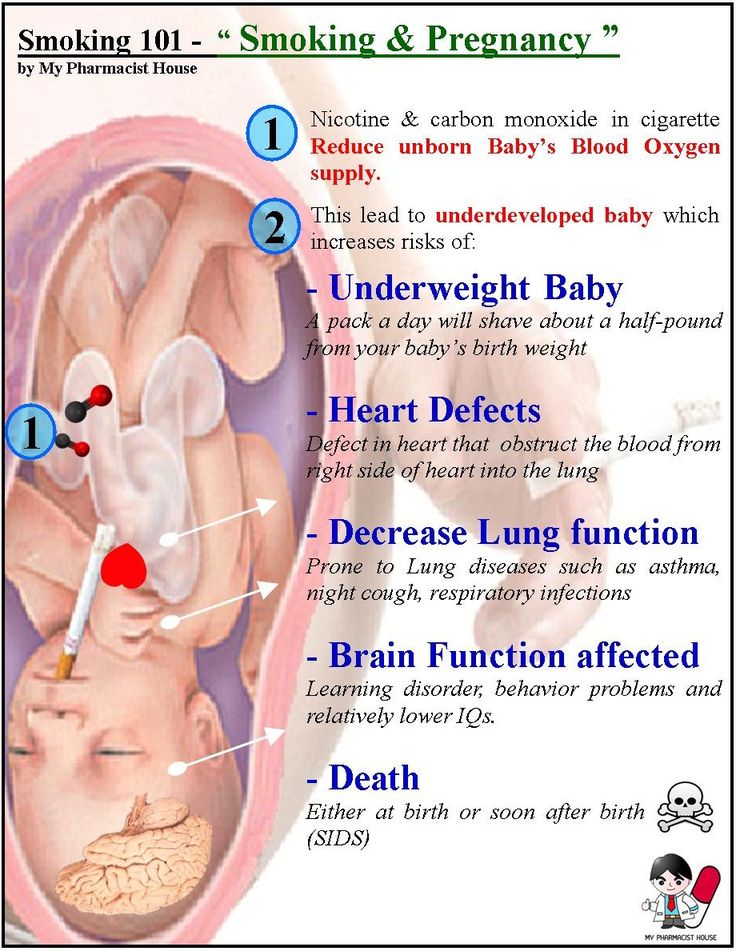
Several factors can contribute to large birth weight. For example:
- the baby's parents' height and stature
- if the baby is a boy (baby boys tend to be larger than baby girls)
- having older siblings (the chance of fetal macrosomia increases with each pregnancy)
- a previous pregnancy in which the baby was large
- being overdue by more than 2 weeks
- if the mother has diabetes during pregnancy
- if the mother gains a lot of weight during pregnancy or is obese
- if the mother is aged 30 or older
In some cases, larger-than-normal birth weight doesn't have a clear cause and can't be explained.
Giving birth to a large baby
Most large babies who weigh more than 4.5kg do not have a difficult birth. But there are still some risks associated with having a big baby.
Labour may take longer and be more likely to involve complications. There's an increased risk of having a forceps or vacuum-assisted delivery or a caesarean, and of birth injury to the mother or baby.
There is a link between fetal macrosomia and shoulder dystocia. Shoulder dystocia occurs during a vaginal birth when the baby's head has been born, but one of the shoulders becomes stuck behind the mother's pelvic bone. The baby's shoulders need to be released quickly so the baby's body can also be born, and they can start breathing.
Shoulder dystocia can happen during any birth. At least half of all babies who experience shoulder dystocia at birth weigh less than 4kg.
Large babies can be born via a normal, vaginal delivery — but it's best to give birth where you can access specialist medical services, just in case things don't go according to plan. Every pregnancy and birth is unique, so talk to your doctor or midwife about the best place for you to give birth.
After the birth of a large baby
Since many large babies are born to mothers with diabetes, some babies will need help regulating their blood sugar after they're born. Later in life, the risk of childhood obesity or being overweight may increase and the baby may develop other problems with their metabolism.
A larger than average baby may need help breathing following the birth, so they may be admitted to the neonatal intensive care unit (NICU) or special care nursery (SCN).
There is also an increased risk of jaundice (yellowing of the skin) among large babies.
Regardless of their size at birth, a baby's weight is always monitored closely after they are born to make sure they are healthy and growing properly. But their weight isn't the only thing that's important. How well they are feeding and the number of wet nappies and poos they produce daily can also indicate that your baby is doing well.
Can you avoid having a large baby?
Often there's nothing you can do to avoid having a large or small baby. But looking after yourself during pregnancy is important for all women. You should consider:
- giving up smoking (if you currently smoke)
- eating a balanced, healthy diet
- maintaining your weight or, if overweight, losing weight before conception if possible
- if you have diabetes, trying to manage it properly
- avoiding alcohol and illegal drugs
Where to seek help
Always talk to your doctor, obstetrician or midwife first if you are concerned about your pregnancy, your own health or the health of your baby.
If you are worried about your baby's growth — or how fetal macrosomia might affect you as a mum — call Pregnancy, Birth and Baby on 1800 882 436 to speak to a maternal child health nurse.
Sources:
Australian Institute of Health and Welfare (Australia's mothers and babies data visualisations), South Australian Perinatal Practice Guidelines (Fetal growth – accelerated), Department of Health (Clinical practice guidelines: Pregnancy care), health.vic (Gestational diabetes), The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Shoulder dystocia)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: September 2020
Back To Top
Related pages
- Labour complications
- Guide to a healthy pregnancy
- Pre-existing diabetes and pregnancy
- Gestational diabetes
- Weight gain in pregnancy
- Check-ups, tests and scans available during your pregnancy
- Routine antenatal tests
- Having a small baby
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Some features, tools or interaction may not work correctly.
Worried about having a big baby? Four things to know about birth weight | Your Pregnancy Matters
As my patients approach their final weeks of pregnancy, they typically start asking questions about how much the baby will weigh and what that means for delivery.
Doctors think about this too. We try to accurately determine the weight of the unborn baby so we can make the best possible birth plan. But predicting birth weight is actually very difficult to do.
In a recent study, one-third of women reported their OB provider told them their baby might be getting “quite large” near the end of pregnancy. In the end, however, only one in five of those women had a baby that weighed more than 8 pounds, 13 ounces or 4000 grams, a common threshold for labeling a baby “large.”
It would be nice to know the exact birth weight of a baby before it’s born – it makes predicting some rare, but serious complications like birth trauma easier. But that’s just not possible, and our estimates of your baby’s size can potentially cause unnecessary stress on mom and lead doctors to intervene when nothing is really necessary.
But that’s just not possible, and our estimates of your baby’s size can potentially cause unnecessary stress on mom and lead doctors to intervene when nothing is really necessary.
Here are some things to think about as you approach the end of pregnancy and are wondering what your baby might weigh and how this could impact your labor and delivery experience:
1. What is considered a ‘big baby’?
Picking an absolute cut-off is tricky. Typically, we consider estimated weights of babies that weigh more than 4500 grams (10 lbs.) as larger than normal (or “macrosomic”). But what we really want to know is whether your baby is too big for your pelvis.
Weight is just one factor doctors consider when we’re estimating the chances of a patient successfully having a vaginal delivery. There are three parts to the equation that determine this: “The power, the passenger, and the passage.”
The “power,” or force of uterine contractions, is something we can only assess when labor begins.
The “passenger” refers to the baby. His or her weight isn’t the only factor – the exact position of the baby within the birth canal also plays an important part in making it out successfully. The direction the head is facing can make all the difference in how easily the baby descends in the birth canal.
“Passage” refers to the anatomy of your pelvis. When doctors do vaginal exams toward the end of the pregnancy, that’s what we’re trying to evaluate: How narrow is the pelvis? Can we reach the tailbone? Do we think this baby will fit through this pelvis?
Like the estimation of fetal size, this isn’t an exact science, but it can help us determine a birth plan for the day of delivery.
2. Ultrasound is not very reliable for estimating fetal weight near term.
For a 9-pound baby, an ultrasound’s predictive accuracy is typically 15 to 20 percent off. Which means we may over- or underestimate by more than a pound. Why is there such a wide range?
Ultrasound uses volumes to calculate fetal weight. It takes measurements of the head, waist circumference and some bones and comes up with an estimate. But it can’t measure the density of the fetal tissues directly.
It takes measurements of the head, waist circumference and some bones and comes up with an estimate. But it can’t measure the density of the fetal tissues directly.
I explain it to my patients like this: I can measure something with ultrasound the size of a brick. That structure will look the same whether made of Styrofoam or stone – but something made of stone obviously weighs a lot more than something made of Styrofoam.
There is a formula for calculating fetal weight based on standard measurements – but not all babies follow the rules for getting the weight accurate! There is no way to know exactly how much a baby is going to weigh until after the baby is born.
3. Who is really at risk for having a big baby?
Certain health and history factors put mothers at increased risk for having a large baby:
- Diabetes, including gestational diabetes, is a concern, especially if the mom’s sugar levels have not been controlled well during pregnancy.
 High glucose levels in mom can cross the placenta and lead to high levels in the fetus. As a response to these high sugar levels, the fetus produces insulin, which stimulates its own growth.
High glucose levels in mom can cross the placenta and lead to high levels in the fetus. As a response to these high sugar levels, the fetus produces insulin, which stimulates its own growth. - Maternal obesity is another big risk factor. The rate of macrosomia has increased over time with rising obesity rates, so we expect to actually see more macrosomic babies in the future.
- History of a previous big baby. The trend is for successive babies to get bigger, not smaller, so this is something we would take into consideration.
If you are not in one of these categories and your health care provider has expressed concern about the size of your baby, I recommend having an honest conversation with him or her about their worries and recommendations.
4. What are the concerns about having a large baby?
We have to consider the possible risks to two patients – both mother and infant. The most serious risk of fetal macrosomia is birth trauma for the baby, especially something called a shoulder dystocia, where after the baby’s head is delivered the rest of his or her body does not deliver easily.
The most serious risk of fetal macrosomia is birth trauma for the baby, especially something called a shoulder dystocia, where after the baby’s head is delivered the rest of his or her body does not deliver easily.
I’ve been in this situation before – it can be pretty frightening, and I completely understand why doctors are quick to recommend a C-section when worried about the possibility for a large baby – it’s an easier way to get the baby out safely.
At the same time, C-sections come with additional risk to the mom and result in additional hospital days, longer recovery periods and added costs. And since our estimates of fetal weight are frequently off, these risks may be unnecessary.
Making a plan that works for you
It is challenging to identify moms and babies that we really need to be concerned about. When doctors label a woman as having a possible “big baby,” we increase the possibility of using interventions during labor such as scheduled C-sections or labor inductions. The average weight of babies that were predicted to be “large” in the study I mentioned earlier was only 7 pounds, 11 ounces – not so big after all.
The average weight of babies that were predicted to be “large” in the study I mentioned earlier was only 7 pounds, 11 ounces – not so big after all.
The recommendations from the American Congress of Obstetricians and Gynecologists are clear. ACOG says ultrasound is no better than a provider’s exam in estimating fetal weight, suspected macrosomia should not be an indication for induction of labor, and planned C-sections shouldn’t be performed unless the estimated fetal weight is 10 pounds or more in diabetic women or 11 pounds or more in other women.
I recommend having an open and frank discussion with your doctor about the clinical information available to you. Discuss the estimated size of your baby, your obstetrical history, your physical exam, and your risk factors. Balance the potential risks and benefits to both you and your baby when making your final decision.
For more information about pregnancy, labor, and delivery, sign up to receive Your Pregnancy Matters email alerts when we publish new stories. You can also make an appointment to see one of our specialists by calling 214-645-8300.
You can also make an appointment to see one of our specialists by calling 214-645-8300.
LARGE FETUS - Article I Clinic of evidence-based medicine NEPLACEBO
Site search Begovaya, 2/3
Personal account
Navigation
For the patient
Personal account
Site search
Kolyadina Anna Alexandrovna
06/30/2021
Surely you have heard how after giving birth a large baby is called a “hero”? In fact, very often (although not always) the birth of a child over 4500 g indicates problems during pregnancy and / or carries risks directly during and after childbirth.
⠀
Gynecologist Anna Kolyadina about a fetus that is too large for her gestational age and, accordingly, a large newborn.
⠀
So, the diagnosis of fetal macrosomia is made if, during a full-term pregnancy, the child was born more than 4000-4500 g (in different countries, different upper limits), or more than 90-95 percentile for a given period.
⠀
Why is fetal macrosomia dangerous?
⠀
For the mother:
🔸Long labor
🔸Increased likelihood of operative vaginal delivery (vacuum extractor) or caesarean section
🔸Ruptures of the vagina, perineum of varying degrees
🔸Risk of postpartum hemorrhage
🔸In rare cases, uterine rupture
⠀
During childbirth for the fetus: manipulations). This situation increases the likelihood of trauma to the baby and mother during childbirth
⠀
For newborns:
🔺 Hypoglycemia (low glucose levels)
🔺 Polycythemia (elevated hematocrit and hemoglobin, which can lead to increased blood viscosity)
🔺 Respiratory problems, risk of perinatal asphyxia
⠀
delayed consequences for children:
a child over 4000 g in a previous pregnancy
✔ Mother's own birth weight over 4000 g
✔ Rarely - some hereditary syndromes
✔ Postterm pregnancy
✔ Maternal obesity
✔ Excessive weight gain during pregnancy (with a normal BMI and weight gain of more than 16 kg, the risk of having a fetus with macrosomia increases by 2. 5 times) : many women who have given birth to large children do not have three main factors (obesity, diabetes and overweight)! Probably, the role of genetic and epigenetic factors is also great.
5 times) : many women who have given birth to large children do not have three main factors (obesity, diabetes and overweight)! Probably, the role of genetic and epigenetic factors is also great.
⠀
❓Why the fetus weighs more than it should
It is believed that the main mechanism for the development of fetal macrosomia is an increased glucose level in a pregnant woman, which, in turn, leads to its increased level in the fetus. As a result, the level of insulin, IGF and growth hormone begins to “storage” fat by the fetus.
Other parameters associated with the risk of macrosomia include elevated triglycerides (⬆️risk) and HDL (⬇️risk) in the mother.
⠀
DIAGNOSIS
⠀
During pregnancy, the large size of the fetus and large weight can be determined using ultrasound (the closer the ultrasound date to childbirth, the more accurate the weight forecast for the newborn)
⠀
During routine visits to the gynecologist, suspicion of a large the fetus can occur when it is palpated and measuring the height of the fundus of the uterus.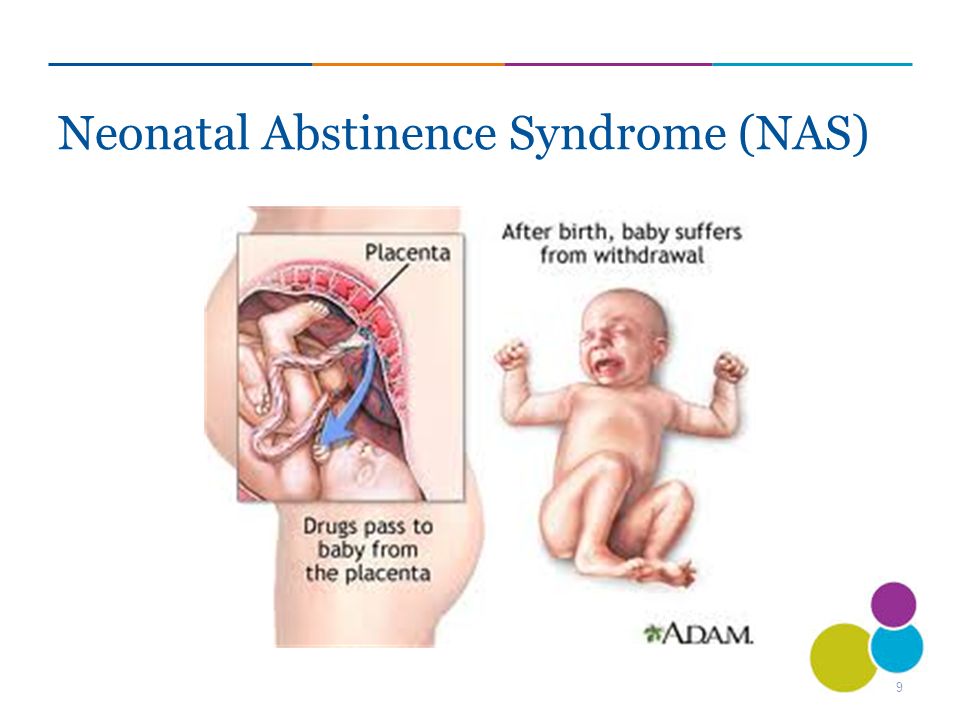 But this method is quite subjective and imprecise.
But this method is quite subjective and imprecise.
⠀
PREVENTION
⠀
All of the above was not intended to scare the expectant mother, but to convey an important message: most macrosomia risk factors can be corrected!
⠀
In case of diabetes or gestational diabetes mellitus, the prevention of fetal macrosomia is GLUCOSE CONTROL and maintenance of its target values.
⠀
In case of obesity, it is worth doing WEIGHT REDUCTION before pregnancy
⠀
In case of normal weight and absence of diabetes, it is worth taking control of WEIGHT GAIN during pregnancy, avoiding going beyond the upper limit of the norm. Adequate regular physical activity will contribute to the favorable course of pregnancy and reduce risks.
⠀
You may be interested in
Sore throat
Every person has experienced sore throat at least once. More often …
Runny nose
“I don’t have a runny nose, just a stuffy nose”, so often …
Nutrition for children
Understanding how much a child’s health depends on the fact that he …
Remember: JavaScript is required for this content .
Open chat
-->If you are waiting for a hero
Main page / Printed materials
Viewings: 43245
“Often in the media there are stories about the birth of baby heroes, weighing five, six and even seven kilograms. It used to be thought that this was a sign of health, but is it really good? Svetlana Leonidovna.
The weight of a newborn from four kilograms is considered large, explains Victoria Panfilova, pediatric endocrinologist, doctor of medical sciences, doctor of the Krasnoyarsk Regional Clinical Center for Maternal and Child Health. The birth of a baby weighing more than four and a half kilograms always causes particular alertness of doctors.
As a rule, it becomes known that the baby will be big by the third semester. This is found out during regular scheduled examinations by an obstetrician-gynecologist leading the pregnancy and during an ultrasound examination. The cause of the appearance of a baby hero may be hereditary factors. For example, the large physique of the child's parents. However, often the large weight of the crumbs can indicate the presence of endocrine problems in the mother or a predisposition to them.
The cause of the appearance of a baby hero may be hereditary factors. For example, the large physique of the child's parents. However, often the large weight of the crumbs can indicate the presence of endocrine problems in the mother or a predisposition to them.
-- There is a form of diabetes that develops during pregnancy - it's gestational diabetes, says Victoria Panfilova. - Before pregnancy, a woman may not suspect that she has this disease. With gestational diabetes, the likelihood of the formation of a large fetus is just high. In addition, the child's pancreas begins to help the mother's body. Excessive insulin production during this period can cause subsequent hypoglycemia in the newborn.
There is no need to panic, the specialist warns, but it is necessary to be attentive to your health. Do not neglect routine medical studies, blood tests. So, the value of venous blood sugar on an empty stomach up to 5.1 mm / l is considered the norm. If this value is higher, then consultation with an endocrinologist is necessary. Also, at the 24-28th week of pregnancy, all pregnant women without a diagnosis of diabetes mellitus undergo an additional study - a glucose tolerance test. A pregnant woman with any form of diabetes should be under the supervision of doctors. The warnings of obstetrician-gynecologists of their patients about moderation in eating are not unfounded. The habit of eating for two, and even harmful sweets, can negatively affect both the well-being of a woman and the health of a child.
Also, at the 24-28th week of pregnancy, all pregnant women without a diagnosis of diabetes mellitus undergo an additional study - a glucose tolerance test. A pregnant woman with any form of diabetes should be under the supervision of doctors. The warnings of obstetrician-gynecologists of their patients about moderation in eating are not unfounded. The habit of eating for two, and even harmful sweets, can negatively affect both the well-being of a woman and the health of a child.
Victoria Panfilova warns that a woman does not need to be overweight, it can cause complications during pregnancy, childbirth, and the risk of metabolic disorders increases.
- Late detection of gestational diabetes is a serious problem. About a quarter of the women who come to us have this disease, - says Pavel Baurov, head of the consultative polyclinic of the regional clinical center for the protection of motherhood and childhood. -- Since 2013, a clinical protocol has been in place for pregnant women to undergo a glucose tolerance test. if the tests showed that the level of sugar in the blood is exceeded. But this rule is not always followed.
if the tests showed that the level of sugar in the blood is exceeded. But this rule is not always followed.
If the expectant mother has no serious illnesses, the baby's heavy weight is still a reason for the close attention of doctors.
-- The weight of a child over 4500 kg at the first birth is an indication for a caesarean section, explains Pavel Baurov. - If a little more than four, then the decision is made depending on the situation: the presence of any obstetric problems, chronic diseases. The largest newborn in my practice is a child weighing 5200. He was born by caesarean section. But there were cases when children weighing 4600 and 4800 were born naturally. But, it should be noted that the mothers there were of the appropriate height and physique.
Heavy birth weight and doctors' fears do not mean that health problems will inevitably arise in the future. And, by the way, it is not a fact that the baby will turn into a giant over the years.
- According to doctors' forecasts, my daughter's birth weight should have been about 4700, - says Julia, mother of nine-year-old Masha, from Krasnoyarsk.