How early can you give birth and the baby survive
the long-term impacts of being born extremely early
- NEWS FEATURE
Babies born before 28 weeks of gestation are surviving into adulthood at higher rates than ever, and scientists are checking in on their health.
- Amber Dance0
- Amber Dance
-
Amber Dance is a freelance journalist in Los Angeles, California.
View author publications
You can also search for this author in PubMed Google Scholar
-
They told Marcelle Girard her baby was dead.
Access options
Subscribe to this journal
Receive 51 print issues and online access
199,00 € per year
only 3,90 € per issue
Learn more
Rent or buy this article
Get just this article for as long as you need it
$39.95
Learn more
Prices may be subject to local taxes which are calculated during checkout
Nature 582, 20-23 (2020)
doi: https://doi.org/10.1038/d41586-020-01517-z
References
Soll, R. & Özek, E. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD000511 (1997).
Article Google Scholar
Soll, R. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD001149 (1998).
Article Google Scholar
British Association of Perinatal Medicine. Perinatal Management of Extreme Preterm Birth Before 27 Weeks of Gestation: A BAPM Framework for Practice (BAPM, 2019).
Google Scholar
Crump, C., Winkleby, M. A., Sundquist, J. & Sundquist, K. J. Am. Med. Assoc. 322, 1580–1588 (2019).
Article Google Scholar
O’Reilly, H., Johnson, S., Ni, Y., Wolke, D. & Marlow, N. Pediatrics 145, e20192087 (2020).
Article PubMed Google Scholar
Garfield, C. F. et al. JAMA Pediatr. 171, 764–770 (2017).
Article PubMed Google Scholar
Saigal, S. et al. Pediatrics 118, 1140–1148 (2006).
Article PubMed Google Scholar
Gire, C. et al. Arch. Dis. Child. 104, 333–339 (2018).
Article PubMed Google Scholar
Bolton, C. E. et al. J. Pediatr. 161, 595–601.e2 (2012).
Article PubMed Google Scholar
Doyle, L. W. et al. Thorax 72, 712–719 (2017).
Article PubMed Google Scholar
Halkerwal, A. et al. Hypertension 75, 211–217 (2019).
Article PubMed Google Scholar
Flahault, A. et al. Hypertension 75, 796–805 (2020).
Article PubMed Google Scholar
Ley, D. et al. J. Pediatr.
 206, 56–65.e8 (2019).
206, 56–65.e8 (2019).Article PubMed Google Scholar
Stalh, A. et al. Lancet 394, 1551–1559 (2019).
Article PubMed Google Scholar
Härkin, P. et al. J. Pediatr. 177, 72–77.e2 (2016).
Article PubMed Google Scholar
Vohr, B. et al. J. Pediatr. 185, 42–48.e1 (2017).
Article PubMed Google Scholar
Liu, Y. et al. J. Pediatr. 200, 91–97.e3 (2018).
Article PubMed Google Scholar
Download references
-
Could baby’s first bacteria take root before birth?
-
The brain, interrupted
-
Insomnia linked to premature birth in study of 3 million mothers
Subjects
- Medical research
- Health care
- Physiology
Latest on:
How Early is Too Early to Deliver?
When I was newly pregnant, I had a miscarriage scare. I worried for the next few months and breathed a giant sigh of relief when I started the second trimester. Then a neighbor went into early labor and I had a new worry. So how early can a baby be born?
I worried for the next few months and breathed a giant sigh of relief when I started the second trimester. Then a neighbor went into early labor and I had a new worry. So how early can a baby be born?
Modern medicine is amazing, especially when it comes to treatments for premature babies. It is nothing short of miraculous, and the advances in understanding have drastically improved the outcome of extremely early deliveries. Here is the current reality:
Baby Born at 22 weeks
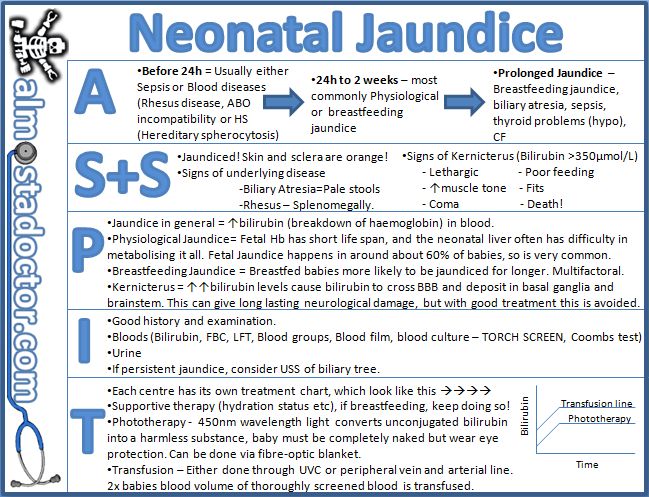
Babies are unlikely to survive at this stage. There is a 14.8% chance of survival for babies born at 22 weeks, but even then, half of these babies have brain damage. As of now, the earliest a baby can be born is 22 and a half weeks. No baby has been successfully delivered before this time. Most babies born at 22 weeks weigh about one pound and do not have functioning lungs, since their airways are not fully developed.
Baby Born at 23-24 weeks
Survival at this stage depends on birth weight and health at birth: 25% of babies survive when born at 23 weeks, and 42 percent survive in the 24th week. Babies born at 23 or 24 weeks depend on a ventilator and around-the-clock care to survive. They have very little body fat and muscle tone. Since they cannot suck and breathe at the same time, they must be fed through an IV.
Babies born at 23 or 24 weeks depend on a ventilator and around-the-clock care to survive. They have very little body fat and muscle tone. Since they cannot suck and breathe at the same time, they must be fed through an IV.
Baby Born at 27 weeks (Extremely early)
90% of babies born who are treated in the neonatal intensive care unit (NICU) will survive to at least one year of age. NICUs are equipped with everything a baby born early might need, such as incubator, overhead heater, all kinds of monitors, feeding pump, IV, and ventilators.
Babies this age deal with the constant threat of hypothermia, low blood sugar, low blood pressure, and infection. They also need help breathing. Though survival rates are extremely high, 25 percent of surviving babies have severe or moderate disabilities, ranging from hearing loss and vision problems to learning disabilities.
Baby Born at 28-31 weeks (Very early)
Premature birth at born at 27 weeks will still require specialized care in the NICU. While they are much stronger than extremely early babies, they are still at risk for hypothermia, low blood sugar, and infection.
While they are much stronger than extremely early babies, they are still at risk for hypothermia, low blood sugar, and infection.
But not all hospitals are equipped with NICUs. Most have a local neonatal unit (LNU) to handle the needs of a stronger but still early baby.
In the absence of a medical problem, babies are healthier the longer they stay in utero. But long-term outcomes are reassuring: only a few of the babies born in weeks 28 and 29 will have problems with eyesight, hearing, movement, or brain development.
Baby Born at 32-33 weeks (Moderately early)
Some babies born at 32 weeks are able to stay with their mothers in a transitional care ward but they still require special care because of problems with breathing, feeding, and infection. Most babies born at this stage weigh between three and four pounds, and are as long as babies at full term (18-19 inches).
Gaining weight is the primary concern for babies born before 34 weeks, since they do not have sufficient body fat to maintain a healthy body temperature. Babies born in this range are also at risk of infection and may have trouble sucking.
Babies born in this range are also at risk of infection and may have trouble sucking.
Baby Born at 34-36 weeks (Early)
Babies born at 34 weeks are incredibly small and strong. They may not need any special treatment or they may need some transitional care depending on how well they are feeding, regulating blood sugar, and blood pressure.
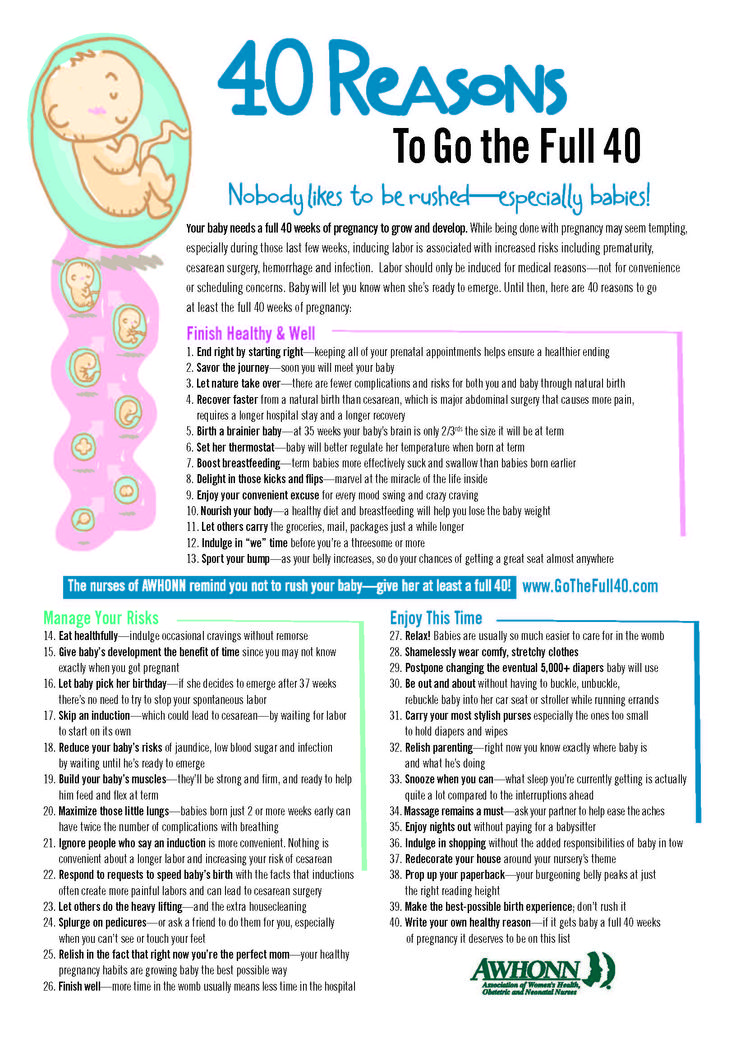
In the last few decades, babies have been considered term at 37 weeks. Since then, many people, including medical professionals, have assumed that not much development occurs after. But new data shows that there is a lot of essential work done in the last few weeks of pregnancy. For example, a baby’s brain at 35 weeks weighs only two-thirds of what it will weigh at 39-40 weeks. Because being born before 39 weeks isn’t without risks, the American Congress of Obstetricians and Gynecologists has redefined the meaning of “term:”
Baby Born at 37-38 weeks (Early term)
Though babies born at 37 weeks were considered full term for many decades, doctors now know that some important development still takes place in weeks 37 and 38. Findings show that babies delivered electively at 37 weeks are four times more likely to spend time in the NICU and have respiratory issues than babies born at 39 or 40 weeks. Babies at this stage still undergo brain, lungs, and liver development.
Findings show that babies delivered electively at 37 weeks are four times more likely to spend time in the NICU and have respiratory issues than babies born at 39 or 40 weeks. Babies at this stage still undergo brain, lungs, and liver development.
Baby Born at 39-40 weeks (Full term)
Babies born at full term are significantly better off than babies born earlier. They breathe better, have gained enough weight to better regulate body temperature, and can suck, swallow, and stay awake long enough to eat.
In my experience, late babies are calmer babies as their nervous systems have had longer to develop. All four of my babies were born after their due date and all of my sister’s babies were born before. Those sweet, early babies are more than fine today. They just needed more patient, attentive care in that first month compared to their cousins.
Still wondering, “How early can you have a baby?” In short, the odds are exponentially better if you deliver after 27 weeks, but a small percentage of babies survive between 22-26 weeks. Rates of survival without complications increase with each week of pregnancy.
Rates of survival without complications increase with each week of pregnancy.
So how can you minimize your chance of premature birth? Here are a few tips:
- Start your pregnancy at a healthy weight and gain the recommended amount of weight during pregnancy.
- Avoid smoking, drugs, and alcohol while pregnant.
- Do everything you can to reduce stress in your life.
- Get vaccinated and protect yourself from infections.
- Visit your doctor for treatment of chronic health problems.
- Wait 18 months to get pregnant between children.
- Avoid heavy lifting and intense physical activity, especially in the later weeks of pregnancy.
Have you delivered a pre-term baby?
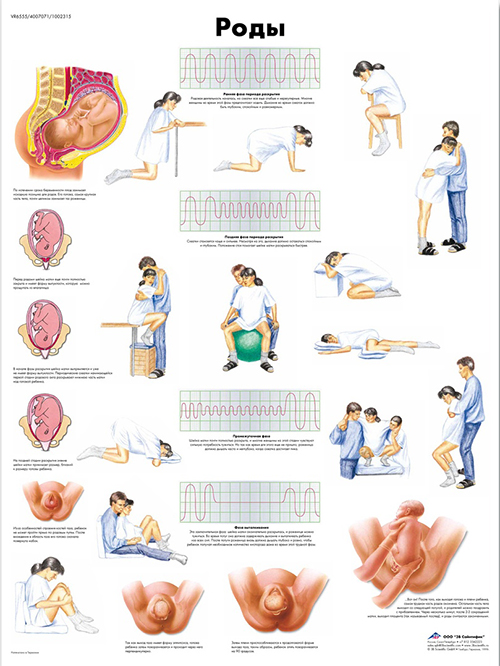
Your baby was born prematurely | Regional Perinatal Center
Premature babies
If your baby is born too early, the joy of having a baby can be overshadowed by health concerns and thoughts about the possible consequences.
Instead of returning home with the baby, holding him and caressing him, you will have to stay in the department, learn to cope with the fear of touching the baby, realize the need for treatment and various manipulations, get used to the complex equipment that surrounds him.
In this situation, not only your baby needs help, you need it too! The best assistants are your loved ones, their love and care, as well as professional advice and recommendations from doctors and psychologists. This section of articles will help you improve your knowledge of preterm infant care, development and nutrition.
Your help for the baby
Previously, parents were often not allowed into the neonatal unit and, especially, into the intensive care unit because of the fear of infection of the baby, but now the contact of the parent with the child is recognized as desirable and is prohibited only in exceptional cases (for example, if parents have acute infections)
Close communication between you and your baby is very important from the first days of his life. Even very immature premature babies recognize the voices and feel the touch of their parents.
Even very immature premature babies recognize the voices and feel the touch of their parents.
The newborn needs this contact. Studies have shown that it greatly contributes to the faster adaptation of an immature child to new conditions and the stabilization of his condition. The baby's resistance to therapy increases, he absorbs large amounts of food and quickly begins to suck on his own. Contact with the child is important for parents. Taking part in the care of the baby, they feel their involvement in what is happening and quickly get used to a new role, especially when they see how he reacts to their presence.
By constantly and attentively observing the baby, parents can notice the smallest changes in his condition before others. In addition, communication in the hospital is a good practice that will undoubtedly come in handy after discharge. For parents, early physical contact with the baby is very valuable, because it allows them to feel him, despite the incubator and other obstacles, and show him their love.
Treatment in the neonatal intensive care unit requires parents to have full confidence in all medical staff.
Nursing premature babies in the hospital
Many premature babies cannot breathe, suckle and regulate their body temperature sufficiently after birth. Only in the last weeks of pregnancy is the maturation of the lungs, gastrointestinal tract, kidneys, brain, which regulates and coordinates the work of all organs and systems.
Fluid loss due to the immaturity of the skin of premature babies and the insufficiency of thermoregulation processes require constant attention. Modern approaches focused on nursing premature babies help to cope with these problems.
Heat regulation incubator
Premature babies are very susceptible to temperature fluctuations. At the same time, clothing can interfere with the monitoring of the baby's condition and its treatment. That is why an incubator is used to provide the conditions necessary for premature babies. It maintains a certain temperature and humidity, which change as the child grows. When the body weight of a premature infant reaches 1500-1700 g, he can be transferred to a heated bed, and after reaching a weight of 2000, most premature babies can do without this support. There are no strict rules here: when nursing children with low body weight, doctors are guided by the severity of the condition of each premature baby and its degree of maturity.
That is why an incubator is used to provide the conditions necessary for premature babies. It maintains a certain temperature and humidity, which change as the child grows. When the body weight of a premature infant reaches 1500-1700 g, he can be transferred to a heated bed, and after reaching a weight of 2000, most premature babies can do without this support. There are no strict rules here: when nursing children with low body weight, doctors are guided by the severity of the condition of each premature baby and its degree of maturity.
In incubators, very young premature babies are placed in special "nests" - soft hemispheres in which the baby feels comfortable and assumes a position close to intrauterine. It must be protected from bright lights and loud noises. For this purpose, special screens and coatings are used.
Critical treatments during the first days of life of premature babies with low and very low birth weight:
Use of an incubator or heated bed.
Oxygen supply for respiratory support.
If necessary, artificial ventilation of the lungs or breathing using the CPAP system.
Intravenous administration of various drugs and fluids.
Carrying out parenteral nutrition with solutions of amino acids, glucose and fat emulsions.
Don't worry: not all premature babies need such extensive treatment!
Mechanical ventilation and CPAP for respiratory support
When it comes to nursing, oxygen supply is of the utmost importance for premature babies. In a child born before the 34-35th week of pregnancy, the ability of the lungs to work independently is not yet sufficiently developed. The use of a constant flow of air with oxygen, which maintains a positive airway pressure (CPAP), leads to an increase in blood oxygen saturation.
This new method made it possible for the majority of even very immature children to do without mechanical ventilation. The need for intubation of children has disappeared: during treatment with CPAP, oxygen is supplied through short tubes - cannulas that are inserted into the nasal passages. CPAP or mechanical ventilation is continued until the lungs can function at full capacity on their own.
CPAP or mechanical ventilation is continued until the lungs can function at full capacity on their own.
In order for the lungs to expand and remain in such a state in the future, a surfactant is needed - a substance that lines the alveoli from the inside and reduces surface tension. Surfactant is produced in sufficient quantities starting from the 34-35th week of pregnancy. Basically, it is by this time that the formation of the lungs is completed. If the baby was born earlier, modern technologies allow the introduction of surfactant into the lungs of premature babies immediately after their birth.
Parenteral nutrition - administering nutrient solutions by vein
Premature babies, especially those born weighing less than 1500 g, are not able to get and absorb enough nutrients, even when fed through a tube. For the rapid growth of the baby, a large amount of nutrition is needed, and the size of the stomach is still very small, and the activity of digestive enzymes is also reduced. Therefore, such children are given parenteral nutrition.
Therefore, such children are given parenteral nutrition.
Special nutrients are injected into a vein using infusion pumps that deliver solutions slowly at a predetermined rate. In this case, amino acids necessary for building proteins, fat emulsions and glucose, which are sources of energy, are used. These substances are also used for the synthesis of a number of hormones, enzymes and other biologically active substances. Additionally, minerals and vitamins are introduced.
Gradually, the volume of enteral nutrition increases, and parenteral nutrition decreases until it is completely canceled.
Premature infants with gastrointestinal disease require parenteral nutrition for a longer period of time.
By the time your grown baby is discharged from the hospital, everything should be well prepared at home. And this applies not only to the environment, clothes and means of caring for the child.
All family members must be ready to receive the baby. Of course, the main care will fall on the shoulders of the parents. Although you have already gained some experience in the hospital, it is important to feel the support of others, especially in the early days.
Of course, the main care will fall on the shoulders of the parents. Although you have already gained some experience in the hospital, it is important to feel the support of others, especially in the early days.
Older children can also help. The discharge of your baby is a great joy that you want to share with all your relatives.
While you are getting used to your new role, it is important that nothing distracts you from communicating with your child. Now all the care and responsibility for the baby lies entirely with you. Everything you need to take care of him should be at hand.
Preparing for discharge from the hospital
Before discharge, you must make sure that:
- Prepared the crib, bath for bathing and a place for changing clothes, preferably a changing table. A crib should be placed in the parents' bedroom, the child should not be left alone even at night. A stroller is also required.
 you have baby milk that was recommended by the doctor before discharge (if the child is on mixed or artificial feeding). As a rule, this is a specialized medical product. You need a certain number of small bottles and teats of the appropriate size, as well as a sterilizer. All premature babies will need pacifiers.
you have baby milk that was recommended by the doctor before discharge (if the child is on mixed or artificial feeding). As a rule, this is a specialized medical product. You need a certain number of small bottles and teats of the appropriate size, as well as a sterilizer. All premature babies will need pacifiers. - You have fully mastered breastfeeding or bottle feeding.
- If your baby is not suckling all the required amount of milk from the breast and is supplementing from a bottle, you have purchased a breast pump that you have learned to use; you may also need it if you have a lot of breast milk.
- You have asked your doctor how often your child's weight should be monitored.
- If your baby still needs medication, you have the required amount at home. And you know exactly how and when to give them to your child.
- You know which warning signs to look out for.
- After the baby is discharged, a pediatrician and a neonatologist will look after the baby, to whom you will give the discharge summary from the hospital.
- You know how the hospital from which your child is being discharged will provide follow-up care after discharge.
- You know which specialists and how often should examine your baby (oculist, neuropathologist, etc.).
- All the emergency phone numbers you need are at your fingertips.
When can a child go home
This question is very difficult to answer because all children are different. The stay in the hospital can last from 6 days to 6 months, depending on the degree of prematurity of the child, the severity of his condition, as well as the presence of certain complications.
Of course, all parents look forward to the moment when the baby can be brought home. Long-term nursing of a premature baby is often a difficult test for you. But we must not forget that safety comes first, and the baby can be discharged home only when the doctors are confident in the stability of his condition. It is certainly in your interest as well.
The rate of increase in body weight and length
Weight gain is the main indicator of the growth of the baby and the adequacy of the treatment. The weight of the child, especially in the first days and weeks of life, is influenced by a number of factors: the presence of milk in the stomach (immediately after feeding), the time of bowel movement, the degree of filling of the bladder, the presence of edema. Therefore, if an edematous child does not gain weight for several days, and perhaps even loses it, do not worry. It should be remembered that children grow unevenly and periods of high weight gain alternate with lower ones. It is better to focus not on weight gain per day, but on the dynamics of this indicator over several days or a week.
It is currently accepted that in the interval corresponding to 28-34 weeks of pregnancy, the normal weight gain of the child is 16-20 g/kg per day. Then it is reduced to 15 g/kg.
It is also important to take into account the rate of increase in body length. With malnutrition, at first the child gains less weight (or even loses it), and with a more pronounced deficiency of nutrients, his growth is also disturbed.
With malnutrition, at first the child gains less weight (or even loses it), and with a more pronounced deficiency of nutrients, his growth is also disturbed.
The weight must not only increase at a certain rate, but must also correspond to the length of the baby. An important parameter characterizing the development of the baby is an increase in the circumference of the head. The brain most actively increases in size during the first 12–18 months of life. But an excessively rapid increase in head circumference, as well as a slowdown in its increase, indicate neurological disorders.
A premature baby can be discharged from the hospital if:
- he is able to independently maintain the required body temperature;
- does not need breathing support and constant monitoring of the work of the respiratory and cardiovascular systems;
- can suck out the required amount of nutrition on its own;
- does not need round-the-clock monitoring and frequent determination of biochemical or other indicators;
- supportive care can be provided at home;
- he will be under the supervision of a local pediatrician and neonatologist at the place of residence.
The decision to discharge home is made for each patient individually. In addition to the state of health of the baby, the degree of preparedness of parents, their ability to provide high-level care for a premature baby is also taken into account.
Feeding a premature baby after discharge
Breastfeeding is the ideal way to feed premature babies.
However, if the baby was born much prematurely and his birth weight did not exceed 1800-2000 g, his high nutritional requirements cannot be met by breastfeeding. The growth rate will be insufficient. Moreover, over time, the content of many nutrients, including protein, in milk decreases. And it is the main material for building organs, and primarily brain tissue. Therefore, proteins must be supplied to the body of a premature infant in the optimal amount.
In addition, premature babies have a significantly increased need for calcium and phosphorus, which are essential for bone formation.
In order for the baby's nutrition to be complete even after being discharged from the hospital, special additives - "enrichers" are introduced into breast milk in a certain amount, already less than in the hospital. They make up for the lack of protein in it, as well as some vitamins and minerals. As a result, the child receives them in the optimal amount. The duration of their use will be determined by your doctor. If there is not enough milk or it does not exist at all, children born prematurely should be transferred to artificial feeding. Complementary feeding of premature babies is carried out with special children's dairy products designed for children with low birth weight. This baby milk is ideally suited to both the ability of immature children to digest and assimilate nutrients, and their needs.
Premature infant milk contains more protein, fat and carbohydrates than term infant milk, resulting in a higher calorie content. In specialized baby milk, the concentration of many minerals is higher, especially iron, zinc, calcium, phosphorus, as well as vitamins, including vitamin D.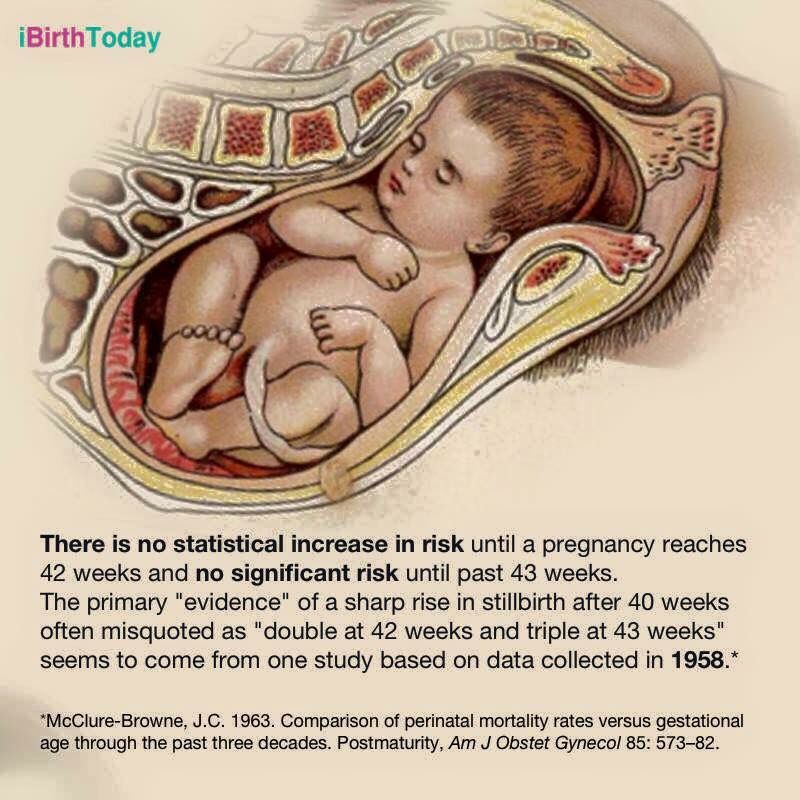 Long-chain polyunsaturated fatty acids of the Omega-3 and Omega-6 classes are introduced into such products, which are necessary for proper development of the brain and organ of vision, as well as nucleotides that contribute to the optimal development of immunity. However, when the child reaches a certain weight (2000-2500 g), you should gradually switch to feeding with standard baby milk, but not completely. Specialized baby milk can be present in the diet of a premature baby for several months. This time, as well as the volume of the product, will be determined by the doctor. He will answer all your questions about how to feed your baby.
Long-chain polyunsaturated fatty acids of the Omega-3 and Omega-6 classes are introduced into such products, which are necessary for proper development of the brain and organ of vision, as well as nucleotides that contribute to the optimal development of immunity. However, when the child reaches a certain weight (2000-2500 g), you should gradually switch to feeding with standard baby milk, but not completely. Specialized baby milk can be present in the diet of a premature baby for several months. This time, as well as the volume of the product, will be determined by the doctor. He will answer all your questions about how to feed your baby.
At present, specialized children's dairy products have been developed and are being used to feed premature babies after discharge from the hospital. In its composition, it occupies an intermediate position between a specialized product for premature babies and regular baby milk. Your baby will be transferred to such baby milk while still in the hospital. You will continue to give it to your child at home, and the doctor, watching him, will tell you when it will be possible to switch to regular standard baby milk. If the baby was born with a very low body weight or is not gaining weight well, special baby milk can be used for a long time - up to 4 months, 6 or even 9months. The beneficial effect of such children's dairy products on the growth and development of the child has been proven in scientific studies.
You will continue to give it to your child at home, and the doctor, watching him, will tell you when it will be possible to switch to regular standard baby milk. If the baby was born with a very low body weight or is not gaining weight well, special baby milk can be used for a long time - up to 4 months, 6 or even 9months. The beneficial effect of such children's dairy products on the growth and development of the child has been proven in scientific studies.
Feeding needs for premature babies
Higher caloric intake because they need to gain weight faster than term babies.
More protein as premature babies grow faster.
More calcium and phosphorus for bone building.
More trace elements and vitamins for growth and development.
A premature baby grows faster than a term baby. Nutrition for such children is calculated taking into account body weight at birth, the age of the baby and its growth rate. As a rule, the calorie content of the daily diet is about 120-130 calories per 1 kg of body weight.
It is very important that your baby continues to gain weight quickly and grow in length after discharge. To do this, feeding premature babies must be carried out using a specialized fortified diet prescribed by a doctor.
▶Prematurity: what causes them ✅ ADONIS MC
Every year, more than 15 million babies are born prematurely. In different countries, they make up from 5 to 18% of the total number of newborns. It is known that preterm birth is a threat to the health of the child due to incomplete intrauterine maturation. Today we asked Alexander Vladimirovich Bogomaz, an obstetrician-gynecologist of the highest category at the ADONIS clinic, to tell us about the causes of preterm birth, their features and methods of pregnancy prolongation.
Alexander Vladimirovich, tell me, which births are considered premature?
- Premature delivery is considered before 37 weeks of gestation, but the critical threshold is 34 weeks. Children who are born before this term are extremely immature. They need intensive care and long-term nursing. If a woman has a risk of preterm birth or certain pathologies, it is desirable that the pregnancy is still prolonged to at least 34 weeks, but preferably up to 37.
Children who are born before this term are extremely immature. They need intensive care and long-term nursing. If a woman has a risk of preterm birth or certain pathologies, it is desirable that the pregnancy is still prolonged to at least 34 weeks, but preferably up to 37.
Tell us about the causes of premature birth. Why do some women give birth on time, while others much earlier?
– There are many reasons for preterm birth, but in some cases they cannot be established. The main ones include chronic diseases of a woman, hormonal disorders in her body, pregnancy pathologies and injuries. Often, premature births occur due to intrauterine infection of the fetus. If a woman had hidden infections of the genitourinary system even before pregnancy, then during the period of gestation, they can become aggravated and transmitted to him.
Is it possible to detect the risk of preterm birth in advance and prolong the pregnancy?
– Yes, now it is possible to predict preterm labor and prolong pregnancy. To do this, control the hormonal background and measure the cervix. In case of shortening, a suture is applied to it or an obstetric pessary is installed. We use different methods to prolong pregnancy, depending on the reasons that increase the risk of preterm birth. With their help, we try to help a woman bring her baby to at least 37 weeks.
To do this, control the hormonal background and measure the cervix. In case of shortening, a suture is applied to it or an obstetric pessary is installed. We use different methods to prolong pregnancy, depending on the reasons that increase the risk of preterm birth. With their help, we try to help a woman bring her baby to at least 37 weeks.
If a woman still has a preterm birth, how do they differ from term birth from the point of view of an obstetrician-gynecologist?
- Premature babies are usually very weak, so you need to try to make childbirth as easy and natural as possible. The doctor should use gentle delivery tactics with minimal interference with the natural process.
If delivery occurs before 34 weeks, the pregnant woman is given a course of dexamethasone injections. It is necessary for the prevention of respiratory disorders in a child. The drug helps to accelerate the maturation of the placenta and internal organs of premature babies.