How do i know if my child has a bowel obstruction
Intussusception (for Parents) - Nemours KidsHealth
What Is Intussusception?
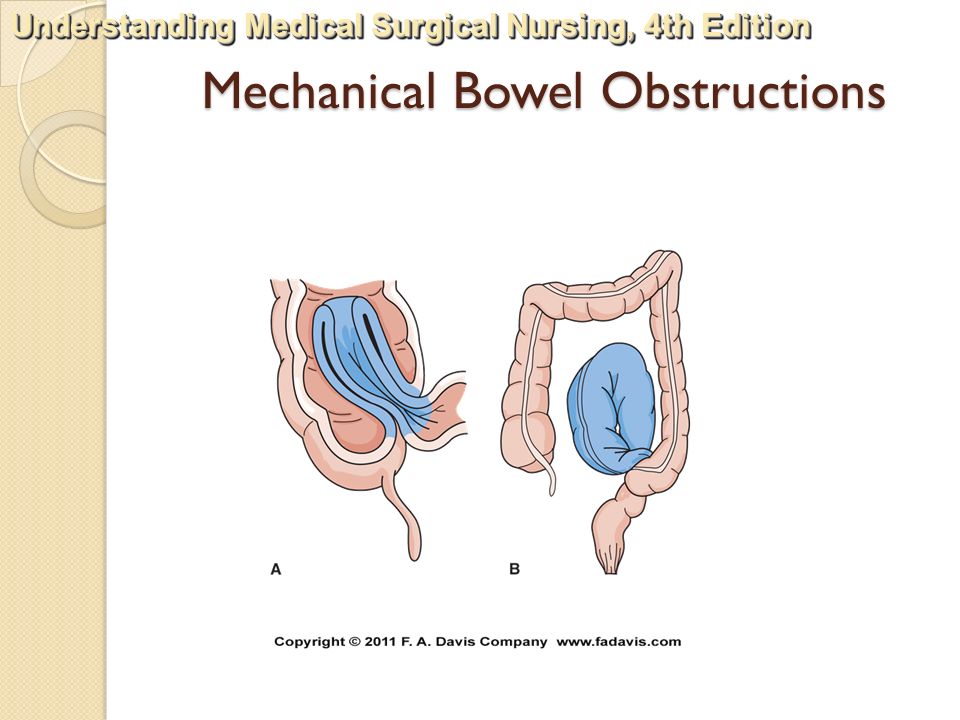
Intussusception (in-tuh-suh-SEP-shun) happens when one part of the bowel slides into the next, much like the pieces of a telescope.
When this "telescoping" happens:
- The flow of fluids and food through the bowel can get blocked.
- The intestine can swell and bleed.
- The blood supply to the affected part of the intestine can get cut off. In time, part of the bowel can die.
Intussusception is a medical emergency that needs care right away. It's the most common abdominal emergency in children under 2 years old.
What Are the Signs & Symptoms of Intussusception?
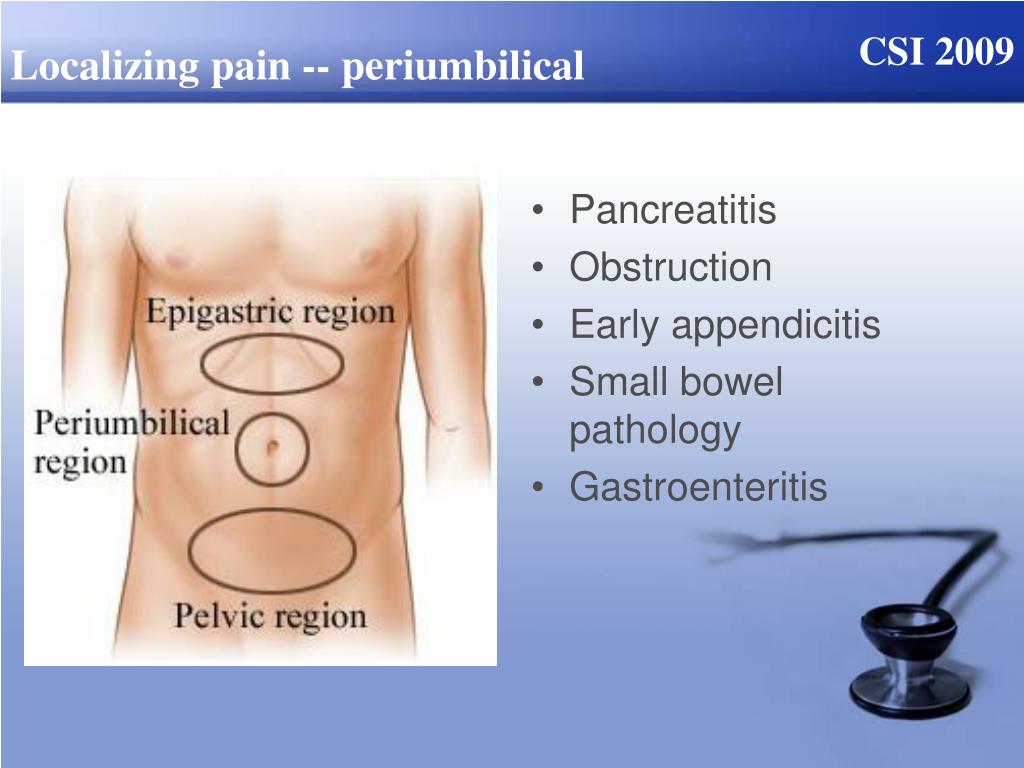
Babies and children with intussusception have intense belly pain that:
- often begins suddenly
- makes the child draw the knees up toward the chest
- makes the child cry very loudly
As the pain eases, the child may stop crying for a while and seem to feel better. The pain usually comes and goes like this, but can be very strong when it returns.
Symptoms also can include:
- a swollen belly
- vomiting
- vomiting up bile, a bitter-tasting yellowish-green fluid
- passing stools (poop) mixed with blood and mucus, known as currant jelly stool
- grunting due to pain
As the illness continues, the child may:
- get weaker
- develop a fever
- appear to go into shock. In this life-threatening problem, a lack of blood flow to the body's organs makes the heart beat quickly and blood pressure drop.
What Causes Intussusception?
Most of the time, doctors don't know what causes intussusception. In some cases, it might follow a recent attack of gastroenteritis (or "stomach flu"). It also can follow a cold or the flu. Bacterial or viral gastrointestinal infections can make the infection-fighting
lymphtissue that lines the intestine swell.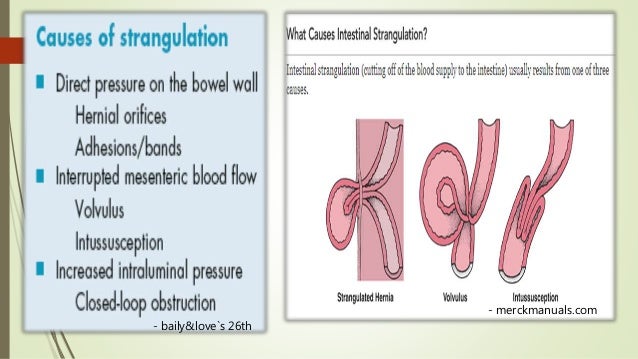 This can cause part of the intestine to get pulled into the other.
This can cause part of the intestine to get pulled into the other.
In kids younger than 3 months old or older than 5, intussusception is more likely to be caused by an underlying condition like enlarged lymph nodes, a tumor, or a blood vessel problem in the intestines.
Intussusception is most common in babies 5 to 9 months old, but older children also can have it. Boys get intussusception more often than girls.
How Is Intussusception Diagnosed?
Doctors usually check for intussusception if a child keeps having periods of pain, drawing up the legs, vomiting, feeling drowsy, or poop with blood and mucus.
During the visit, the doctor will:
- do an exam, paying special attention to the belly, which may be swollen or tender to the touch. Sometimes the doctor can feel the part of the intestine that's involved.
- ask about the child's health, family health, any medicines taken, and any allergies
How Is Intussusception Treated?
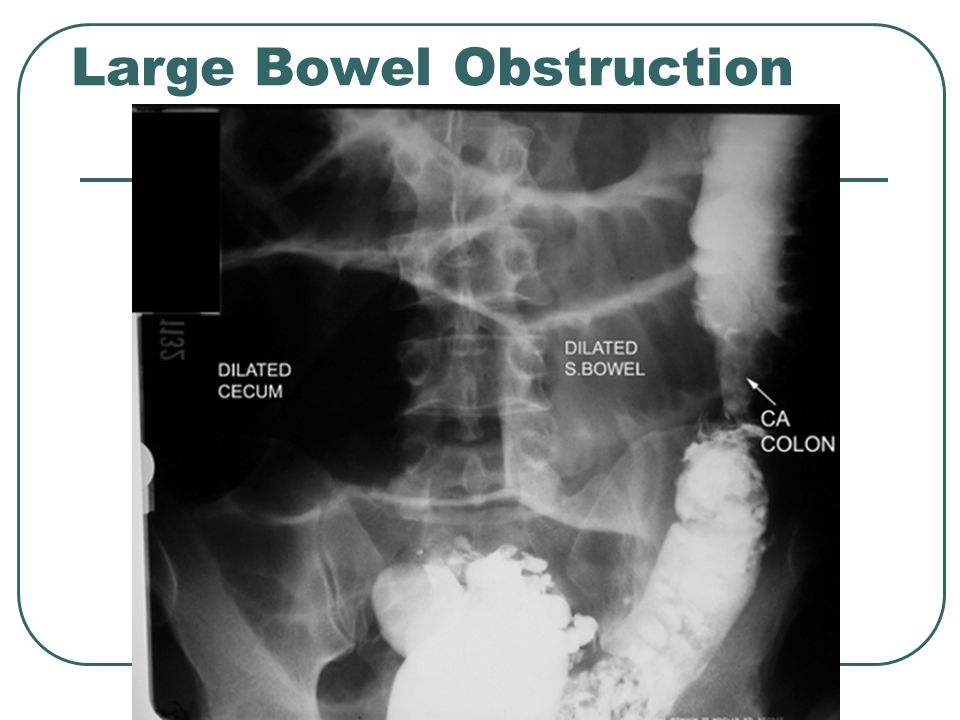
If the doctor suspects intussusception, the child may be sent to an emergency room (ER). Usually, doctors there will ask a pediatric surgeon to see the child right away. The ER doctor might order an abdominal ultrasound or X-ray, which can sometimes show a blockage in the intestines. If the child looks very sick, suggesting damage to the intestine, the surgeon may take the child to the operating room right away to fix the blocked bowel.
Usually, doctors there will ask a pediatric surgeon to see the child right away. The ER doctor might order an abdominal ultrasound or X-ray, which can sometimes show a blockage in the intestines. If the child looks very sick, suggesting damage to the intestine, the surgeon may take the child to the operating room right away to fix the blocked bowel.
Two kinds of enemas often can diagnose and treat intussusception at the same time:
- In an air enema, doctors place a small soft tube in the rectum (where poop comes out) and pass air though the tube. The air travels into the intestines and outlines the bowels on the X-rays. If there's intussusception, it shows the telescoping piece in the intestine. At the same time, the pressure of the air unfolds the inside-out section of bowel and cures the blockage.
- In a barium enema, a liquid mixture called barium is used instead of air to fix the blockage in the same way.
Both types of enema are very safe, and children usually do very well. Most children treated with the enema do not need surgery. In a few children, intussusception can return, usually within 72 hours of the procedure. They may need a repeat enema.
Most children treated with the enema do not need surgery. In a few children, intussusception can return, usually within 72 hours of the procedure. They may need a repeat enema.
A child will need surgery if the intestine is torn, an enema doesn't work, or the child is too sick for an enema. This is often the case in older children. Then, surgeons will try to fix the obstruction. But if too much damage has been done, they may need to remove that part of the bowel.
After treatment, the child will stay in the hospital and get IV feedings until they can eat and have normal bowel function. Doctors will watch the child to make sure that the intussusception does not come back. Some babies also may get antibiotics to prevent infection.
When Should I Call the Doctor?
Intussusception is a medical emergency. Call your doctor or get emergency medical help right away if your child has any symptoms of intussusception, such as:
- repeated crampy belly pain
- vomiting
- drowsiness
- passing of currant jelly stool
Most children treated within the first 24 hours recover completely with no problems.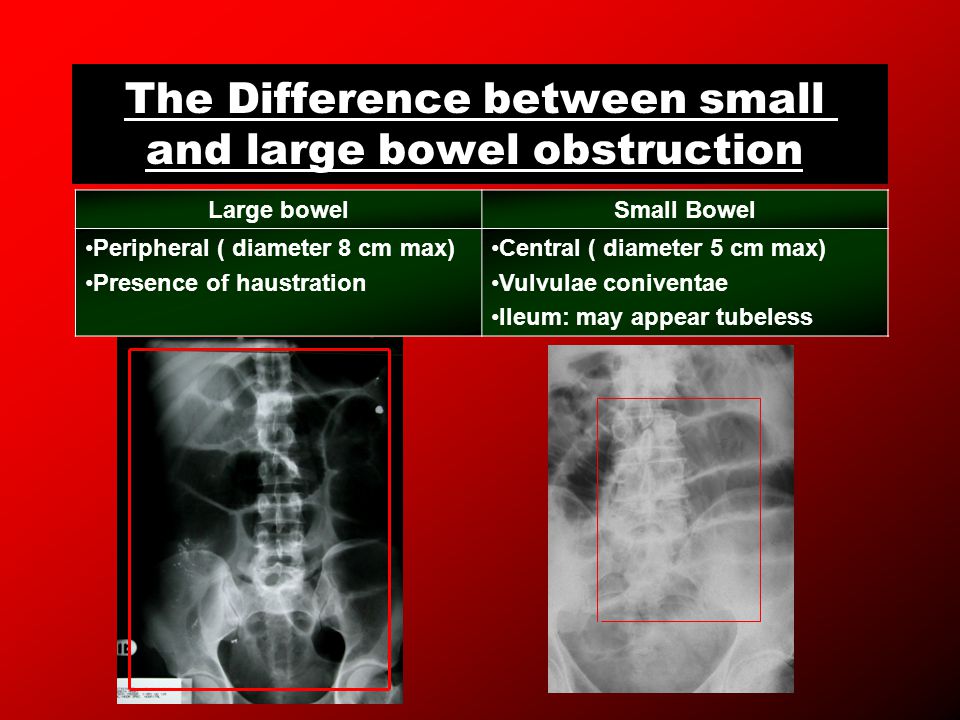 But untreated intussusception can cause serious problems that get worse quickly. So it's important to get help right away — every second counts.
But untreated intussusception can cause serious problems that get worse quickly. So it's important to get help right away — every second counts.
Pediatric Small Bowel Obstruction Clinical Presentation: History, Physical Examination
Overman RE Jr, Hilu MH, Gadepalli SH. Early postoperative small bowel obstruction after appendectomy because of staples in pediatric patients. J Surg Res. 2020 Oct. 254:314-7. [QxMD MEDLINE Link].
Kitagawa S, Miqdady M. Intussusception in children. UpToDate. 2014; Accessed: October 2015.
Wright TN, Fallat ME. Intussusception. In: Holcomb GW III, Murphy JP, St Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia: Elsevier; 2020. ch 46.
Mansour AM, El Koutby M, El Barbary MM, et al. Enteric viral infections as potential risk factors for intussusception.
 J Infect Dev Ctries. 2013 Jan 15. 7(1):28-35. [QxMD MEDLINE Link]. [Full Text].
J Infect Dev Ctries. 2013 Jan 15. 7(1):28-35. [QxMD MEDLINE Link]. [Full Text].Nylund CM, Denson LA, Noel JM. Bacterial enteritis as a risk factor for childhood intussusception: a retrospective cohort study. J Pediatr. 2010 May. 156(5):761-5. [QxMD MEDLINE Link].
Okimoto S, Hyodo S, Yamamoto M, Nakamura K, Kobayashi M. Association of viral isolates from stool samples with intussusception in children. Int J Infect Dis. 2011 Sep. 15(9):e641-5. [QxMD MEDLINE Link].
Weintraub ES, Baggs J, Duffy J, et al. Risk of intussusception after monovalent rotavirus vaccination. N Engl J Med. 2014 Feb 6. 370(6):513-9. [QxMD MEDLINE Link]. [Full Text].
Patel MM, Lopez-Collada VR, Bulhoes MM, et al. Intussusception risk and health benefits of rotavirus vaccination in Mexico and Brazil.
 N Engl J Med. 2011 Jun 16. 364(24):2283-92. [QxMD MEDLINE Link]. [Full Text].
N Engl J Med. 2011 Jun 16. 364(24):2283-92. [QxMD MEDLINE Link]. [Full Text].Abbo O, Pinnagoda K, Micol LA, Beck-Popovic M, Joseph JM. Osteosarcoma metastasis causing ileo-ileal intussusception. World J Surg Oncol. 2013. 11(1):188. [QxMD MEDLINE Link]. [Full Text].
Laje P, Stanley CA, Adzick NS. Intussusception after pancreatic surgery in children: a case series. J Pediatr Surg. 2010 Jul. 45(7):1496-9. [QxMD MEDLINE Link].
Nikolic H, Palcevski G, Saina G, Persic M. Chronic intussusception in children caused by Ascaris lumbricoides. Wien Klin Wochenschr. 2011 May. 123(9-10):294-6. [QxMD MEDLINE Link].
Vestergaard H, Westergaard T, Wohlfahrt J, Pipper C, Melbye M. Association between intussusception and tonsil disease in childhood.
 Epidemiology. 2008 Jan. 19(1):71-4. [QxMD MEDLINE Link].
Epidemiology. 2008 Jan. 19(1):71-4. [QxMD MEDLINE Link]. van Lier MG, Mathus-Vliegen EM, Wagner A, van Leerdam ME, Kuipers EJ. High cumulative risk of intussusception in patients with Peutz-Jeghers syndrome: time to update surveillance guidelines?. Am J Gastroenterol. 2011 May. 106(5):940-5. [QxMD MEDLINE Link].
Snyder CL, Escouno M, Esposito C. Inguinal hernia. In: Holcomb GW III, Murphy JP, St Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, Pa: Elsevier; 2020. ch 50.
Rajput A, Gauderer MW, Hack M. Inguinal hernias in very low birth weight infants: incidence and timing of repair. J Pediatr Surg. 1992 Oct. 27(10):1322-4. [QxMD MEDLINE Link].
de Goede B, Verhelst J, van Kempen BJ, et al. Very low birth weight is an independent risk factor for emergency surgery in premature infants with inguinal hernia.
 J Am Coll Surg. 2015 Mar. 220(3):347-52. [QxMD MEDLINE Link].
J Am Coll Surg. 2015 Mar. 220(3):347-52. [QxMD MEDLINE Link]. Lakshminarayanan B, Hughes-Thomas AO, Grant HW. Epidemiology of adhesions in infants and children following open surgery. Semin Pediatr Surg. 2014 Dec. 23(6):344-8. [QxMD MEDLINE Link].
Nasir AA, Abdur-Rahman LO, Bamigbola KT, Oyinloye AO, Abdulraheem NT, Adeniran JO. Is non-operative management still justified in the treatment of adhesive small bowel obstruction in children?. Afr J Paediatr Surg. 2013 Jul-Sep. 10(3):259-64. [QxMD MEDLINE Link].
Tsao KJ, St Peter SD, Valusek PA, et al. Adhesive small bowel obstruction after appendectomy in children: comparison between the laparoscopic and open approach. J Pediatr Surg. 2007 Jun. 42(6):939-42. [QxMD MEDLINE Link].
Kihne M, Ramanujam TM, Sithasanan N. Mesocolic hernia: a rare cause of intestinal obstruction in childhood. Med J Malaysia. 2006 Jun. 61(2):251-3. [QxMD MEDLINE Link].
Villalona GA, Diefenbach KA, Touloukian RJ. Congenital and acquired mesocolic hernias presenting with small bowel obstruction in childhood and adolescence. J Pediatr Surg. 2010 Feb. 45(2):438-42. [QxMD MEDLINE Link].
Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. 2011 Jan 20. 364(3):255-64. [QxMD MEDLINE Link].
Leys CM. Meckel diverticulum. In: Holcomb GW III, Murphy JP, St Peter SD, Gatti JM eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, Pa: Elsevier; 2020. ch 40.
Foley PT, Sithasanan N, McEwing R, et al. Enteric duplications presenting as antenatally detected abdominal cysts: is delayed resection appropriate?.
 J Pediatr Surg. 2003 Dec. 38(12):1810-3. [QxMD MEDLINE Link].
J Pediatr Surg. 2003 Dec. 38(12):1810-3. [QxMD MEDLINE Link]. Fusco JC, Malek MM, Gittes GK. Lesions of the pancreas. In: Holcomb GW III, Murphy JP, St Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, Pa: Elsevier; 2020. ch 46.
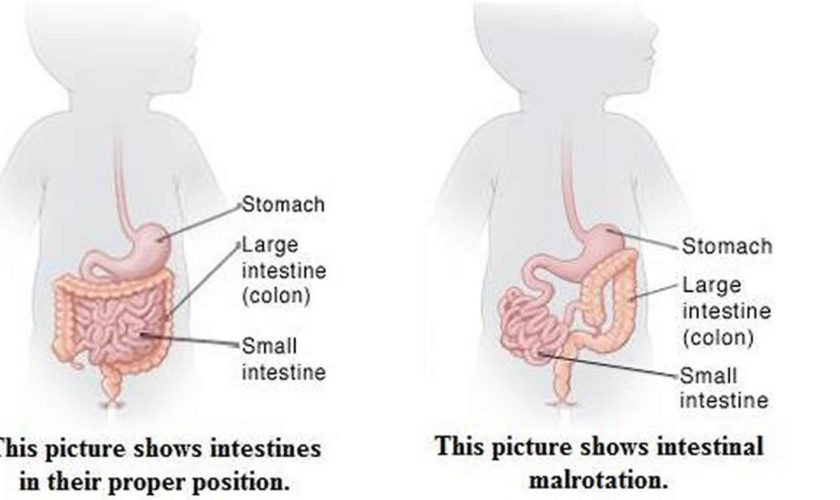
Bonasso PC, Dassinger MS, Smith SD. Malrotation. In: Holcomb GW III, Murphy JP, St Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, Pa: Elsevier; 2020. ch 31.
Karrer FM, Ogle S. Pediatic duodenal atresia. Medscape Drugs & Diseases. Updated: July 20, 2020. Available at http://emedicine.medscape.com/article/932917-overview. Accessed: September 21, 2020.
Lewis N, Glick P. Pediatric duodenal atresia and stenosis surgery. Medscape Drugs & Diseases.
 Updated: April 7, 2020. Available at http://emedicine.medscape.com/article/935748-overview. Accessed: September 21, 2020.
Updated: April 7, 2020. Available at http://emedicine.medscape.com/article/935748-overview. Accessed: September 21, 2020.Chang YJ, Yan DC, Lai JY, et al. Strangulated small bowel obstruction in children. J Pediatr Surg. 2017 Aug. 52(8):1313-17. [QxMD MEDLINE Link].
Moss RL, Kalish LA, Duggan C, et al. Clinical parameters do not adequately predict outcome in necrotizing enterocolitis: a multi-institutional study. J Perinatol. 2008 Oct. 28(10):665-74. [QxMD MEDLINE Link].
Berman L, Moss RL. Necrotizing enterocolitis: an update. Semin Fetal Neonatal Med. 2011 Jun. 16(3):145-50. [QxMD MEDLINE Link].
Zhang Y, Ortega G, Camp M, Osen H, Chang DC, Abdullah F. Necrotizing enterocolitis requiring surgery: outcomes by intestinal location of disease in 4371 infants.
 J Pediatr Surg. 2011 Aug. 46(8):1475-81. [QxMD MEDLINE Link].
J Pediatr Surg. 2011 Aug. 46(8):1475-81. [QxMD MEDLINE Link]. Wright NJ, Thyoka M, Kiely EM, et al. The outcome of critically ill neonates undergoing laparotomy for necrotising enterocolitis in the neonatal intensive care unit: a 10-year review. J Pediatr Surg. 2014 Aug. 49(8):1210-4. [QxMD MEDLINE Link].
Duro D, Kalish LA, Johnston P, et al. Risk factors for intestinal failure in infants with necrotizing enterocolitis: a Glaser Pediatric Research Network study. J Pediatr. 2010 Aug. 157(2):203-208.e1. [QxMD MEDLINE Link]. [Full Text].
Lee N, Kim SG, Lee YJ, et al. Congenital internal hernia presented with life threatening extensive small bowel strangulation. Pediatr Gastroenterol Hepatol Nutr. 2013 Sep. 16(3):190-4. [QxMD MEDLINE Link]. [Full Text].
Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. 1978 Jan. 187(1):1-7. [QxMD MEDLINE Link]. [Full Text].
Rastogi S, Olmez I, Bhutada A, Rastogi D. Drop in platelet counts in extremely preterm neonates and its association with clinical outcomes. J Pediatr Hematol Oncol. 2011 Dec. 33(8):580-4. [QxMD MEDLINE Link].
Hooker RL, Hernanz-Schulman M, Yu C, et al. Radiographic evaluation of intussusception: utility of left-side-down decubitus view. Radiology. 2008 Sep. 248(3):987-94. [QxMD MEDLINE Link]. [Full Text].
Roskind CG, Ruzal-Shapiro CB, Dowd EK, et al. Test characteristics of the 3-view abdominal radiograph series in the diagnosis of intussusception. Pediatr Emerg Care. 2007 Nov. 23(11):785-9.
 [QxMD MEDLINE Link].
[QxMD MEDLINE Link]. Dadlani A, Lal S, Shahani B, Ali M. Ultrasonography for the diagnosis of intussusception in children: an experience from Pakistan. Cureus. 2020 Aug 11. 12(8):e9656. [QxMD MEDLINE Link]. [Full Text].
Pazo A, Hill J, Losek JD. Delayed repeat enema in the management of intussusception. Pediatr Emerg Care. 2010 Sep. 26(9):640-5. [QxMD MEDLINE Link].
Sizemore AW, Rabbani KZ, Ladd A, et al. Diagnostic performance of the upper gastrointestinal series in the evaluation of children with clinically suspected malrotation. Pediatr Radiol. 2008 May. 38(5):518-28. [QxMD MEDLINE Link].
Brandt ML. Intestinal malrotation. UpToDate. Available at https://www.uptodate.com/contents/intestinal-malrotation-in-children. 2014; Accessed: October 2015.
Gul A, Tekoglu G, Aslan H, et al. Prenatal sonographic features of esophageal and ileal duplications at 18 weeks of gestation. Prenat Diagn. 2004 Dec 15. 24(12):969-71. [QxMD MEDLINE Link].
Dordelmann M, Rau GA, Bartels D, et al. Evaluation of portal venous gas detected by ultrasound examination for diagnosis of necrotising enterocolitis. Arch Dis Child Fetal Neonatal Ed. 2009 May. 94(3):F183-7. [QxMD MEDLINE Link].
Faingold R, Daneman A, Tomlinson G, et al. Necrotizing enterocolitis: assessment of bowel viability with color doppler US. Radiology. 2005 May. 235(2):587-94. [QxMD MEDLINE Link].
Task Force for Children's Surgical Care. Optimal resources for children's surgical care in the United States. J Am Coll Surg. 2014 Mar.
 218(3):479-87, 487.e1-4. [QxMD MEDLINE Link].
218(3):479-87, 487.e1-4. [QxMD MEDLINE Link]. Tareen F, Ryan S, Avanzini S, Pena V, Mc Laughlin D, Puri P. Does the length of the history influence the outcome of pneumatic reduction of intussusception in children?. Pediatr Surg Int. 2011 Jun. 27(6):587-9. [QxMD MEDLINE Link].
Ramachandran P, Gupta A, Vincent P, et al. Air enema for intussusception: is predicting the outcome important?. Pediatr Surg Int. 2008 Mar. 24(3):311-3. [QxMD MEDLINE Link].
Whitehouse JS, Gourlay DM, Winthrop AL, Cassidy LD, Arca MJ. Is it safe to discharge intussusception patients after successful hydrostatic reduction?. J Pediatr Surg. 2010 Jun. 45(6):1182-6. [QxMD MEDLINE Link].
Linden AF, Raiji MT, Kohler JE, et al. Evaluation of a water-soluble contrast protocol for nonoperative management of pediatric adhesive small bowel obstruction.
 J Pediatr Surg. 2019 Jan. 54(1):184-8. [QxMD MEDLINE Link].
J Pediatr Surg. 2019 Jan. 54(1):184-8. [QxMD MEDLINE Link]. Fraser JD, Aguayo P, Ho B, et al. Laparoscopic management of intussusception in pediatric patients. J Laparoendosc Adv Surg Tech A. 2009 Aug. 19(4):563-5. [QxMD MEDLINE Link].
Kao C, Tseng SH, Chen Y. Laparoscopic reduction of intussusception in children by a single surgeon in comparison with open surgery. Minim Invasive Ther Allied Technol. 2011 May. 20(3):141-5. [QxMD MEDLINE Link].
Le CK, Cooper W. Volvulus. In: StatPearls. August 13, 2020. Treasure Island (FL): StatPearls Publishing. [QxMD MEDLINE Link]. [Full Text].
Draus JM Jr, Foley DS, Bond SJ. Laparoscopic Ladd procedure: a minimally invasive approach to malrotation without midgut volvulus. Am Surg.
 2007 Jul. 73(7):693-6. [QxMD MEDLINE Link].
2007 Jul. 73(7):693-6. [QxMD MEDLINE Link]. Tsumura H, Ichikawa T, Murakami Y, et al. Laparoscopic adhesiolysis for recurrent postoperative small bowel obstruction. Hepatogastroenterology. 2004 Jul-Aug. 51(58):1058-61. [QxMD MEDLINE Link].
Banieghbal B, Beale PG. Minimal access approach to jejunal atresia. J Pediatr Surg. 2007 Aug. 42(8):1362-4. [QxMD MEDLINE Link].
Kozlov Y, Novogilov V, Yurkov P, Podkamenev A, Weber I, Sirkin N. Keyhole approach for repair of congenital duodenal obstruction. Eur J Pediatr Surg. 2011 Mar. 21(2):124-7. [QxMD MEDLINE Link].
Jawaheer J, Khalil B, Plummer T, et al. Primary resection and anastomosis for complicated meconium ileus: a safe procedure?. Pediatr Surg Int. 2007 Nov. 23(11):1091-3.
 [QxMD MEDLINE Link].
[QxMD MEDLINE Link]. Kandpal DK, Siddharth S, Balan S, Chowdhary SK. Intestinal obstruction in a premature baby: endoscopic diagnosis and management by minimal access surgery. J Indian Assoc Pediatr Surg. 2013 Jul. 18(3):118-20. [QxMD MEDLINE Link]. [Full Text].
Chan KW, Lee KH, Wong HY, et al. Laparoscopic excision of Meckel's diverticulum in children: what is the current evidence?. World J Gastroenterol. 2014 Nov 7. 20(41):15158-62. [QxMD MEDLINE Link]. [Full Text].
Bales C, Liacouras CA. Intestinal atresia, stenosis and malrotation. In: Kliegman RM, Stanton BF, St Geme JW, Schor NF, eds. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, Pa: Saunders; ch 330.
Ruscher KA, Fisher JN, Hughes CD, et al. National trends in the surgical management of Meckel's diverticulum.
 J Pediatr Surg. 2011 May. 46(5):893-6. [QxMD MEDLINE Link].
J Pediatr Surg. 2011 May. 46(5):893-6. [QxMD MEDLINE Link]. Wang SM, Huang FC, Wu CH, Ko SF, Lee SY, Hsiao CC. Ileocecal Burkitt's lymphoma presenting as ileocolic intussusception with appendiceal invagination and acute appendicitis. J Formos Med Assoc. 2010 Jun. 109(6):476-9. [QxMD MEDLINE Link]. [Full Text].
Esposito F, Ambrosio C, De Fronzo S, et al. Fluoroscopy-guided hydrostatic reduction of intussusception in infancy: role of pharmacological premedication. Radiol Med. 2015 Jun. 120(6):549-56. [QxMD MEDLINE Link].
Ikossi DG, Shaheen R, Mallory B. Laparoscopic femoral hernia repair using umbilical ligament as plug. J Laparoendosc Adv Surg Tech A. 2005 Apr. 15(2):197-200. [QxMD MEDLINE Link].
Chan KL, Hui WC, Tam PK.
 Prospective randomized single-center, single-blind comparison of laparoscopic vs open repair of pediatric inguinal hernia. Surg Endosc. 2005 Jul. 19(7):927-32. [QxMD MEDLINE Link].
Prospective randomized single-center, single-blind comparison of laparoscopic vs open repair of pediatric inguinal hernia. Surg Endosc. 2005 Jul. 19(7):927-32. [QxMD MEDLINE Link]. Boley SJ, Cahn D, Lauer T, Weinberg G, Kleinhaus S. The irreducible ovary: a true emergency. J Pediatr Surg. 1991 Sep. 26(9):1035-8. [QxMD MEDLINE Link].
Mboyo A, Goura E, Massicot R, et al. An exceptional cause of intestinal obstruction in a 2-year-old boy: strangulated hernia of the ileum through Winslow's foramen. J Pediatr Surg. 2008 Jan. 43(1):e1-3. [QxMD MEDLINE Link].
Gingalewski C, Lalikos J. An unusual cause of small bowel obstruction: herniation through a defect in the falciform ligament. J Pediatr Surg. 2008 Feb. 43(2):398-400. [QxMD MEDLINE Link].
El-Gohary Y, Alagtal M, Gillick J. Long-term complications following operative intervention for intestinal malrotation: a 10-year review. Pediatr Surg Int. 2010 Feb. 26(2):203-6. [QxMD MEDLINE Link].
Chesley PM, Melzer L, Bradford MC, Avansino JR. Association of anorectal malformation and intestinal malrotation. Am J Surg. 2015 May. 209 (5):907-11; discussion 912. [QxMD MEDLINE Link].
Kargl S, Wagner O, Pumberger W. Volvulus without malposition--a single-center experience. J Surg Res. 2015 Jan. 193(1):295-9. [QxMD MEDLINE Link].
Prasad A, Chadha R. Intestinal obstruction. In: Gupta DK, ed. Pediatric Surgery: Diagnosis and Management. New Delhi, India: Jaypee Import; 2009.
Li M, Ren J, Zhu W, et al. Long intestinal tube splinting really prevents recurrence of postoperative adhesive small bowel obstruction: a study of 1,071 cases.
 Am J Surg. 2015 Feb. 209(2):289-96. [QxMD MEDLINE Link].
Am J Surg. 2015 Feb. 209(2):289-96. [QxMD MEDLINE Link]. Ohno Y, Kanematsu T. Annular pancreas causing localized recurrent pancreatitis in a child: report of a case. Surg Today. 2008. 38(11):1052-5. [QxMD MEDLINE Link].
Morgan JA, Young L, McGuire W. Pathogenesis and prevention of necrotizing enterocolitis. Curr Opin Infect Dis. 2011 Jun. 24(3):183-9. [QxMD MEDLINE Link].
Henry MC, Moss RL. Neonatal necrotizing enterocolitis. Semin Pediatr Surg. 2008 May. 17(2):98-109. [QxMD MEDLINE Link].
Fisher JG, Bairdain S, Sparks EA, et al. Serious congenital heart disease and necrotizing enterocolitis in very low birth weight neonates. J Am Coll Surg. 2015 Jun. 220(6):1018-26.e14. [QxMD MEDLINE Link].
Dilli D, Aydin B, Fettah ND, et al. The propre-save study: effects of probiotics and prebiotics alone or combined on necrotizing enterocolitis in very low birth weight infants. J Pediatr. 2015 Mar. 166(3):545-51.e1. [QxMD MEDLINE Link].
Lau CS, Chamberlain RS. Probiotic administration can prevent necrotizing enterocolitis in preterm infants: a meta-analysis. J Pediatr Surg. 2015 Aug. 50(8):1405-12. [QxMD MEDLINE Link].
Tayman C, Tonbul A, Kahveci H, et al. C5a, a complement activation product, is a useful marker in predicting the severity of necrotizing enterocolitis. Tohoku J Exp Med. 2011. 224(2):143-50. [QxMD MEDLINE Link].
Young CM, Kingma SD, Neu J. Ischemia-reperfusion and neonatal intestinal injury. J Pediatr. 2011 Feb. 158(2 suppl):e25-8. [QxMD MEDLINE Link].
Autmizguine J, Hornik CP, Benjamin DK Jr, et al, for the Best Pharmaceuticals for Children Act—Pediatric Trials Network Administrative Core Committee. Anaerobic antimicrobial therapy after necrotizing enterocolitis in VLBW infants. Pediatrics. 2015 Jan. 135(1):e117-25. [QxMD MEDLINE Link]. [Full Text].
Heida FH, Hulscher JB, Schurink M, et al. Intestinal fatty acid-binding protein levels in necrotizing enterocolitis correlate with extent of necrotic bowel: results from a multicenter study. J Pediatr Surg. 2015 Jul. 50(7):1115-8. [QxMD MEDLINE Link].
Kumar KJ, Kumar MG, Shyamala P, Kumar MP. Meckel's diverticulitis causing intestinal obstruction in a 3 month old infant. J Res Med Sci. 2013 Sep. 18(9):826. [QxMD MEDLINE Link].
Nose S, Okuyama H, Sasaki T, Nishimura M.
 Torsion of Meckel's diverticulum in a child. Case Rep Gastroenterol. 2013 Jan. 7(1):14-8. [QxMD MEDLINE Link]. [Full Text].
Torsion of Meckel's diverticulum in a child. Case Rep Gastroenterol. 2013 Jan. 7(1):14-8. [QxMD MEDLINE Link]. [Full Text].Javid P, Pauli E. Meckel’s diverticulum. UpToDate. Jan 2014; Accessed: October 2015.
Nam SH, Koo SH, Chung ML, Jung YJ, Lim YJ. Congenital antral web in premature baby. Pediatr Gastroenterol Hepatol Nutr. 2013 Mar. 16(1):49-52. [QxMD MEDLINE Link]. [Full Text].
Herndon CD, Rink RC, Cain MP, et al. In situ Malone antegrade continence enema in 127 patients: a 6-year experience. J Urol. 2004 Oct. 172(4 pt 2):1689-91. [QxMD MEDLINE Link].
Ladd WE, Gross RE. Surgical treatment of duplication of the alimentary tract: enterogenous cysts, enteric cysts, or ileum duplex. Surg Gynecol Obstet. 1940. 70:295-307.
Ksia A, Zitouni H, Zrig A, et al. Pyloric atresia: a report of ten patients. Afr J Paediatr Surg. 2013 Apr-Jun. 10(2):192-4. [QxMD MEDLINE Link].
Wetherill C, Sutcliffe J. Hirschsprung disease and anorectal malformation. Early Hum Dev. 2014 Dec. 90(12):927-32. [QxMD MEDLINE Link].
Mark I, Richard M. Emergent evaluation of the child with acute abdominal pain. UpToDate. 2014; Accessed: October 2015.
Rosenbaum J, Alex G, Simpson D, Catto-Smith A. Luminal view of an intussusception captured by capsule endoscopy. J Pediatr Gastroenterol Nutr. 2011 Aug. 53(2):127. [QxMD MEDLINE Link].
Fazio VW, Cohen Z, Fleshman JW, et al. Reduction in adhesive small-bowel obstruction by Seprafilm adhesion barrier after intestinal resection.
 Dis Colon Rectum. 2006 Jan. 49(1):1-11. [QxMD MEDLINE Link].
Dis Colon Rectum. 2006 Jan. 49(1):1-11. [QxMD MEDLINE Link]. Shah U, Shafiq Y, Khan MA. Gastrograffin use in distal intestinal obstruction syndrome of cystic fibrosis. J Ayub Med Coll Abbottabad. 2007 Jan-Mar. 19(1):58-60. [QxMD MEDLINE Link].
Yagci G, Kaymakcioglu N, Can MF, et al. Comparison of Urografin versus standard therapy in postoperative small bowel obstruction. J Invest Surg. 2005 Nov-Dec. 18(6):315-20. [QxMD MEDLINE Link].
Ekenze SO, Mgbor SO. Childhood intussusception: the implications of delayed presentation. Afr J Paediatr Surg. 2011 Jan-Apr. 8(1):15-8. [QxMD MEDLINE Link].
Kaiser AD, Applegate KE, Ladd AP. Current success in the treatment of intussusception in children. Surgery. 2007 Oct. 142(4):469-75; discussion 475-7.
 [QxMD MEDLINE Link].
[QxMD MEDLINE Link]. Abbas S, Bissett IP, Parry BR. Oral water soluble contrast for the management of adhesive small bowel obstruction. Cochrane Database Syst Rev. 2007 Jul 18. CD004651. [QxMD MEDLINE Link].
Rao SC, Basani L, Simmer K, Samnakay N, Deshpande G. Peritoneal drainage versus laparotomy as initial surgical treatment for perforated necrotizing enterocolitis or spontaneous intestinal perforation in preterm low birth weight infants. Cochrane Database Syst Rev. 2011 Jun 15. CD006182. [QxMD MEDLINE Link].
James DC, Lessen R. Position of the American Dietetic Association: promoting and supporting breastfeeding. J Am Diet Assoc. 2009 Nov. 109(11):1926-42. [QxMD MEDLINE Link].
Neilson JP. Probiotics for prevention of necrotizing enterocolitis in preterm infants.
 Obstet Gynecol. 2008 May. 111(5):1202-4. [QxMD MEDLINE Link].
Obstet Gynecol. 2008 May. 111(5):1202-4. [QxMD MEDLINE Link]. Alfaleh K, Anabrees J, Bassler D, Al-Kharfi T. Probiotics for prevention of necrotizing enterocolitis in preterm infants. Cochrane Database Syst Rev. 2011 Mar 16. CD005496. [QxMD MEDLINE Link].
Haque KN, Pammi M. Pentoxifylline for treatment of sepsis and necrotizing enterocolitis in neonates. Cochrane Database Syst Rev. 2011 Oct 5. CD004205. [QxMD MEDLINE Link].
Sola JE, Tepas JJ 3rd, Koniaris LG. Peritoneal drainage versus laparotomy for necrotizing enterocolitis and intestinal perforation: a meta-analysis. J Surg Res. 2010 Jun 1. 161(1):95-100. [QxMD MEDLINE Link].
Stevenson DK, Kerner JA, Malachowski N, Sunshine P. Late morbidity among survivors of necrotizing enterocolitis.
 Pediatrics. 1980 Dec. 66(6):925-7. [QxMD MEDLINE Link].
Pediatrics. 1980 Dec. 66(6):925-7. [QxMD MEDLINE Link]. Minney-Smith CA, Levy A, Hodge M, et al. Intussusception is associated with the detection of adenovirus C, enterovirus B and rotavirus in a rotavirus vaccinated population. J Clin Virol. 2014 Dec. 61(4):579-84. [QxMD MEDLINE Link].
Pammi M, Abrams SA. Oral lactoferrin for the prevention of sepsis and necrotizing enterocolitis in preterm infants. Cochrane Database Syst Rev. 2015 Feb 20. 2:CD007137. [QxMD MEDLINE Link].
Ogle SB, Nichol PF, Ostlie DJ. Duodenal and intestinal atresia and stenosis. In: Holcomb GW III, Murphy JP, St Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, Pa: Elsevier; 2020. ch 30.
Acute intestinal obstruction: causes, symptoms, treatment
Violation of the passage of contents through the intestines or adhesions leads to such an unpleasant problem as intestinal obstruction.
Causes
Acute intestinal obstruction is an independent functional disorder, a consequence of other pathologies or injuries. The problem can be caused by:
- peritonitis,
- heavy metal salt poisoning,
- neoplasms,
- jumps in intra-abdominal pressure,
- gallstones,
- infectious diseases,
- a sharp decrease in body weight,
- vascular thrombosis,
- disorders of the stomach.
Acute obstruction: classification
- If hemodynamics, innervation (connection of internal organs with the central nervous system) is disturbed, then they speak of mechanical intestinal obstruction.
- Intestinal obstruction associated with compression of the intestinal lumen and compression of blood vessels is called strangulation. nine0014
- If adhesions are the cause, the patient is diagnosed with acute adhesive ileus.
- The result of paralysis, paresis - the so-called paralytic ileus.
Intestinal obstruction can be decompensated (no stool, signs of detoxification, anemia are pronounced), subcompensated (persistent constipation, the colon is significantly expanded, stool - with the help of enema, a large amount of laxative) and compensated (irregular stool, effective solution to the problem of constipation with laxatives). nine0003
Symptoms of intestinal obstruction
Symptoms affect both the gastrointestinal tract itself and other organs and systems of the body:
- Cramping pains in the abdomen (pain is not “tied” to eating).
- Constipation.
- Increased flatulence, bloating.
- Vomiting (often, but not always - may be absent in colonic obstruction).
- Rapid pulse.
- Pale skin.
- Without a medical diagnosis, a person can decide that the problem is an exacerbation of chronic colitis, an infectious disease, and even heart problems.
Diagnosis
The main methods of diagnosis are auscultation and percussion of the abdomen.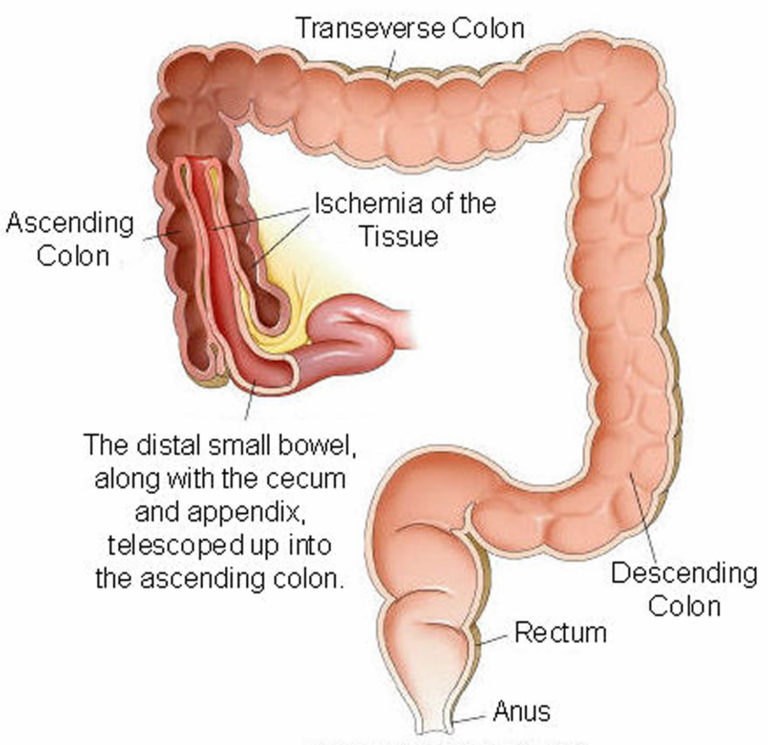 In addition, important information for making a diagnosis can be obtained as a result of colonoscopy and fluoroscopy - always with a contrast agent.
In addition, important information for making a diagnosis can be obtained as a result of colonoscopy and fluoroscopy - always with a contrast agent.
Laboratory diagnostics is also important, especially a general and detailed biochemical blood test, including the determination of the level of chlorides, leukocytes and nitrogen. nine0003
The patient is also given a urine test. If cylinders, protein and blood elements appear in the urine, the disease progresses.
Treatment
Treatment is aimed at restoring intestinal patency, simulating motility, combating spasms and gas formation, and restoring electrolytes in the body.
In the initial stages, therapeutic methods are used, with the progression of the disease, severe obstruction, volvulus of the intestine and closure of the lumen, surgical intervention is required. nine0003
In case of intestinal volvulus, nodulation, an operation is performed to eliminate the node. If there are no signs of peritonitis, but the disease progresses strongly, a colostomy and hemicolonectomy are performed. If peritonitis has developed, surgeons perform a transversostomy.
If peritonitis has developed, surgeons perform a transversostomy.
Prevention
A significant problem is the recurrence of the disease. To prevent them, it is important to remember about prevention. What it includes:
- Small meals and elimination of foods that cause gas in the intestines. nine0014
- Regular biochemical blood test, abdominal ultrasound and colonoscopy.
- Injury avoidance.
If signs of intestinal obstruction reappear, it is important to see a doctor immediately. It is also important to deal with the prevention of adhesion formation for everyone who has a tendency to form adhesions. These people are a special risk group.
You can undergo intestinal diagnostics and receive high-quality surgical treatment for intestinal obstruction at the 5th clinical hospital in Minsk. Attentive and experienced doctors work here to help defeat the disease. nine0003
Acute intestinal obstruction - symptoms, treatment, diagnosis
Acute intestinal obstruction is a life-threatening pathological condition that is characterized by a violation of the passage of the contents of the gastrointestinal tract from the stomach to the anus. It is not an independent disease and is a complication of a variety of diseases. However, having arisen, intestinal obstruction develops according to a single scenario and is accompanied by typical clinical manifestations. In the absence of timely treatment, the prognosis for intestinal obstruction is extremely unfavorable. nine0003
It is not an independent disease and is a complication of a variety of diseases. However, having arisen, intestinal obstruction develops according to a single scenario and is accompanied by typical clinical manifestations. In the absence of timely treatment, the prognosis for intestinal obstruction is extremely unfavorable. nine0003
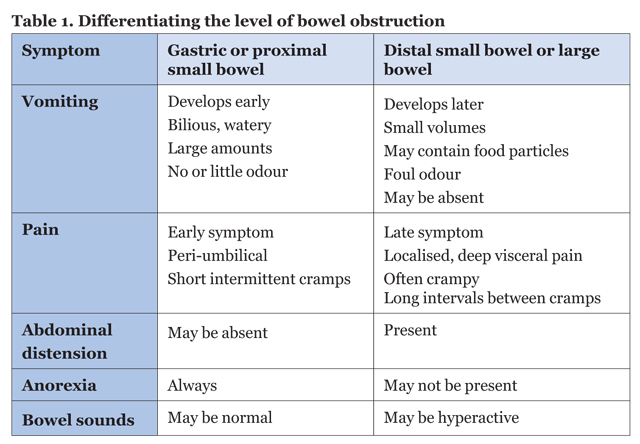
Of great importance is the level at which intestinal obstruction occurred. The higher the obstacle arises, the more difficult it is, the more vigorous therapeutic measures it requires.
Types of intestinal obstruction
It is customary to distinguish between dynamic intestinal obstruction, when the motor function of the intestinal wall is disturbed (i.e., peristalsis is disturbed and the movement of the contents through the intestine stops) and mechanical intestinal obstruction (in this case, mechanical blockage of the intestine occurs at some level). nine0003
Mechanical obstruction is much more common and can develop due to blockage of the intestine by a foreign body, tumor, feces, as well as due to compression or infringement of the intestine from the outside during adhesions in the abdominal cavity, volvulus or formation of nodes. Dynamic intestinal obstruction can develop with diffuse peritonitis of any etiology, with long-term biliary or renal colic, after surgery on the abdominal organs, in case of poisoning with salts of heavy metals, as well as injuries and tumors of the brain and spinal cord (when the innervation of the intestinal wall is disturbed) . nine0003
Dynamic intestinal obstruction can develop with diffuse peritonitis of any etiology, with long-term biliary or renal colic, after surgery on the abdominal organs, in case of poisoning with salts of heavy metals, as well as injuries and tumors of the brain and spinal cord (when the innervation of the intestinal wall is disturbed) . nine0003
Sign up for a consultation The first consultation is free!
I agree with the agreement for the processing of personal data
Symptoms
- Severe, cramping or persistent abdominal pain that occurs suddenly, regardless of food intake, and does not have a specific localization.
- Bloating.
- Intractable vomiting (the higher the level of obstruction, the more pronounced vomiting). nine0014
- Retention of stools and gases (with high obstruction, there may first be stool due to bowel emptying below the level of the obstruction).
Diagnostics
Plain radiography, ultrasound of the abdominal organs, MSCT can be performed to confirm the diagnosis.
If signs of intestinal obstruction are detected, to clarify the localization of the process, radiography is performed with oral administration of a radiopaque substance. A colonoscopy (an endoscopic method for examining the large intestine) and other additional studies may also be performed. nine0003
Treatment
In most cases, urgent surgery is needed.
However, all types of dynamic obstruction are subject to conservative treatment, which includes ensuring the patency of the gastrointestinal tract with the help of enemas, removal of intestinal contents with a nasogastric or nasointestinal tube, correction of water and electrolyte disorders, control of hemodynamics, normalization of peristalsis, detoxification and antibiotic therapy. nine0003
Any questions?
Leave the phone -
and we will call you back
Our leading specialists
All specialists
Evseev Maxim Alexandrovich
Vladykin Alexey Leonidovich
Alekseev Mikhail Sergeevich
Fedotov Stanislav Viktorovich
Balaryov Anton Sergeevich
Efimkina Jennet Orazmammetovna
nine0002 Zatsarinny Vladimir ViktorovichRozumny Ilya Arkadyevich
Titkov Boris Evgenievich
Benefits of the Hospital Center
Individual treatment regimen for each patient
For each patient, on a mandatory basis, even at the pre-hospital stage, an individual treatment regimen is developed, taking into account all the characteristics of the body: age, health status, medical history, etc. – this approach allows minimizing the risks both during the operation and in the postoperative period, and as a result, to ensure the fastest possible rehabilitation with a minimum stay in the hospital. nine0003
– this approach allows minimizing the risks both during the operation and in the postoperative period, and as a result, to ensure the fastest possible rehabilitation with a minimum stay in the hospital. nine0003
Multidisciplinary approach
The medical staff of the Hospital Center is a single team made up of doctors - experts in different specialties, which allows for a multidisciplinary approach. We treat a patient, seeing before us not a list of his diseases, but a person whose problems are interconnected and interdependent. The therapeutic measures taken are always aimed at improving the overall health, well-being and quality of life of the patient, and are not limited to eliminating the symptoms of a particular disease. nine0003
Surgical treatment of any level of complexity
Operating doctors of the Hospital Center have advanced and high-tech methods of performing operations. The combination of highly qualified doctors and innovative equipment allows for surgical treatment of the highest level of complexity.
High-tech, minimally invasive methods of treatment
The basis of the treatment methodology carried out at the Hospital Center is the principles of minimizing risks for the patient and the fastest possible rehabilitation. nine0003
The implementation of this approach is possible only with the use of the most high-tech techniques, modern equipment and the latest achievements of medical science.
The qualifications of doctors, combined with modern equipment, allows us to successfully implement this approach to treatment.
Fast-track surgery
Fast-track is a comprehensive technique that allows you to minimize the length of the patient's stay in the hospital without compromising the quality of treatment. nine0003
The approach is based on minimizing surgical trauma, reducing the risk of postoperative complications and accelerated recovery after surgical operations, which provides our patients with a minimum hospital stay.
Even complex operations such as cholecystectomy, thanks to this approach, require a hospital stay of no more than 3 days.
Personal medical supervision in the postoperative period
To completely exclude the development of possible complications, all patients, regardless of the complexity of the operation, spend the early postoperative period in the intensive care unit under the individual supervision of a resuscitator. nine0003
The transfer of the patient to the ward is carried out only in the absence of even the smallest possible risks.
Informing relatives 24/7
We are as open as possible and take care not only about the patient, but also about his relatives. Information about the health status of patients is provided to relatives seven days a week, 24 hours a day.
Visiting patients is also possible at any convenient time.
Highly comfortable single and double rooms
Patients are offered spacious, comfortable rooms for single and double occupancy, equipped with everything necessary for rest and recovery.
In the children's department, our little patients are accommodated together with their parents.