Cleft lip is an example of a congenital disorder
Cleft lip | Definition, Causes, Surgery, & Facts
- Related Topics:
- congenital disorder cleft palate
See all related content →
Top Questions
What causes a cleft lip?
A cleft lip is a relatively common congenital deformity that is sometimes familial. Behaviours and environmental factors during pregnancy may also be causes, including smoking, alcohol consumption, drug use, nutritional deficiencies, certain medications, and viral infections. Some populations, particularly in Asia, are more prone to cleft lip than others.
What is a cleft lip?
A cleft lip is a fissure in the lip beneath the nostril that results when the central to medial upper lip fails to fuse properly during the second month of prenatal life. It may be unilateral or bilateral.
How is cleft lip surgery done?
Cleft lip surgery consists of freeing the tissues in the cleft margins and then suturing together the tissue layers.
cleft lip, relatively common congenital deformity in which the central to medial upper lip fails to fuse properly during the second month of prenatal life, resulting in a fissure in the lip beneath the nostril. Once colloquially known as harelip, cleft lip may be unilateral or bilateral. It may take the form of anything from a small pit to a complete fissure extending the entire vertical length of the lip into the nostril, and it may occur alone or in conjunction with cleft palate (a fissure in the roof of the mouth). Most cleft lips exhibit an associated deformity of the nose, wherein the cartilage and other tissues of the nose are malformed. Many cleft lips are also associated with a cleft of the gum (alveolus), which can range from a small notch of the gum to a complete separation of all tissues, including the bone.
Cleft lip is sometimes familial, and it is a frequent finding in certain congenital disorders. Risk for cleft lip may be influenced by race, being particularly common among Asians. The development of cleft lip may also be associated with exposure to environmental factors during pregnancy, including smoking, alcohol consumption, drug use, nutritional deficiencies (e.g., folate deficiency), certain medications (e.g., seizure medications), and viral infections.
The development of cleft lip may also be associated with exposure to environmental factors during pregnancy, including smoking, alcohol consumption, drug use, nutritional deficiencies (e.g., folate deficiency), certain medications (e.g., seizure medications), and viral infections.
Babies born with a cleft lip but with a normal palate generally are able to feed without significant difficulty. Dental abnormalities are common, characterized by malaligned teeth or fewer than normal teeth. Some individuals with unrepaired or poorly repaired clefts of the lip also experience psychological difficulties, which may be aggravated by teasing and ostracization. Self-esteem may be affected negatively and result in the child’s withdrawal from social activities. The psychological problems incurred by children with unrepaired or improperly repaired clefts can be serious and debilitating.
Cleft lip may be diagnosed before birth through ultrasound and is readily apparent at birth. Surgery to correct the condition usually is performed at about three months of age, although it may be performed slightly earlier or later. Surgery consists of freeing the tissues in the cleft margins and then suturing together the tissue layers (e.g., skin, muscle). Some surgeons also treat deformities of the nose at the time of the cleft-lip repair. Children with cleft lip often require specialized dental care and psychological intervention.
Surgery consists of freeing the tissues in the cleft margins and then suturing together the tissue layers (e.g., skin, muscle). Some surgeons also treat deformities of the nose at the time of the cleft-lip repair. Children with cleft lip often require specialized dental care and psychological intervention.
W. Geoff Williams
Facts about Cleft Lip and Cleft Palate
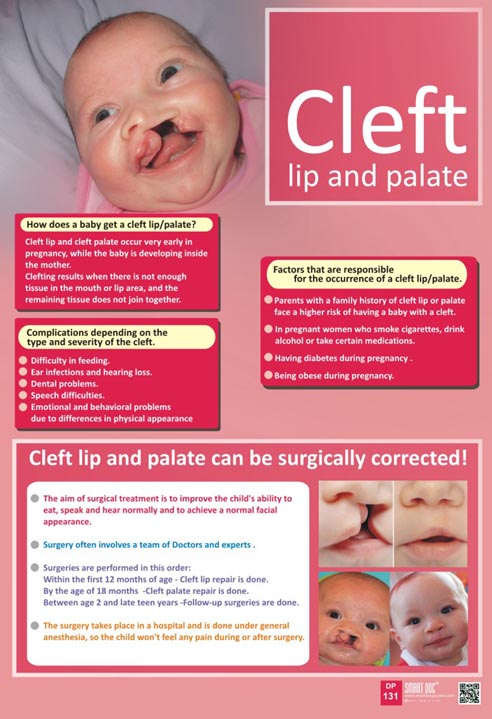
Cleft lip and cleft palate are birth defects that occur when a baby’s lip or mouth do not form properly during pregnancy. Together, these birth defects commonly are called “orofacial clefts”.
Click here to view a larger image
Click here to view a larger image
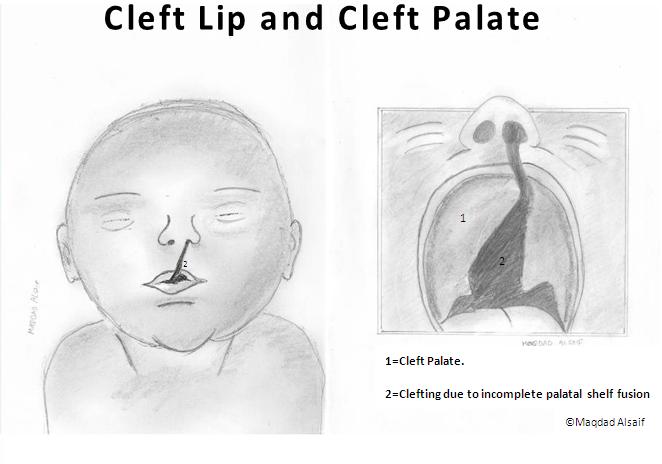
What is Cleft Lip?
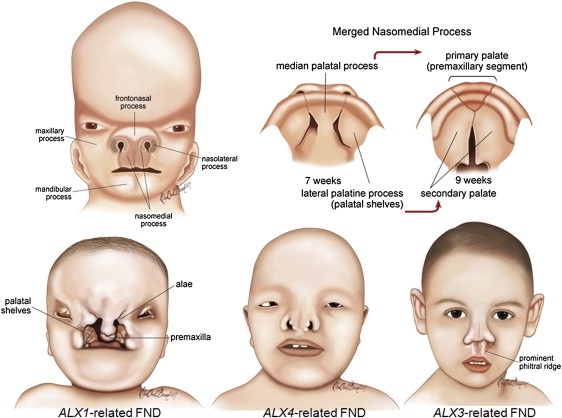
The lip forms between the fourth and seventh weeks of pregnancy. As a baby develops during pregnancy, body tissue and special cells from each side of the head grow toward the center of the face and join together to make the face. This joining of tissue forms the facial features, like the lips and mouth. A cleft lip happens if the tissue that makes up the lip does not join completely before birth. This results in an opening in the upper lip. The opening in the lip can be a small slit or it can be a large opening that goes through the lip into the nose. A cleft lip can be on one or both sides of the lip or in the middle of the lip, which occurs very rarely. Children with a cleft lip also can have a cleft palate.
A cleft lip happens if the tissue that makes up the lip does not join completely before birth. This results in an opening in the upper lip. The opening in the lip can be a small slit or it can be a large opening that goes through the lip into the nose. A cleft lip can be on one or both sides of the lip or in the middle of the lip, which occurs very rarely. Children with a cleft lip also can have a cleft palate.
What is Cleft Palate?
The roof of the mouth (palate) is formed between the sixth and ninth weeks of pregnancy. A cleft palate happens if the tissue that makes up the roof of the mouth does not join together completely during pregnancy. For some babies, both the front and back parts of the palate are open. For other babies, only part of the palate is open.
Other Problems
Children with a cleft lip with or without a cleft palate or a cleft palate alone often have problems with feeding and speaking clearly and can have ear infections. They also might have hearing problems and problems with their teeth.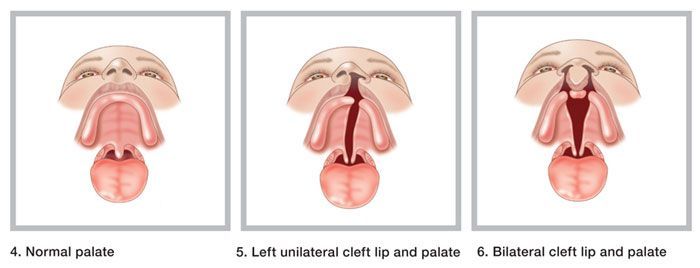
How Many Babies are Born with Cleft Lip/Cleft Palate?
- About 1 in every 1,600 babies is born with cleft lip with cleft palate in the United States.
- About 1 in every 2,800 babies is born with cleft lip without cleft palate in the United States.
- About 1 in every 1,700 babies is born with cleft palate in the United States.1
Causes and Risk Factors
The causes of orofacial clefts among most infants are unknown. Some children have a cleft lip or cleft palate because of changes in their genes. Cleft lip and cleft palate are thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
Like the many families of children with birth defects, CDC wants to find out what causes them. Understanding the factors that are more common among babies with a birth defect will help us learn more about the causes.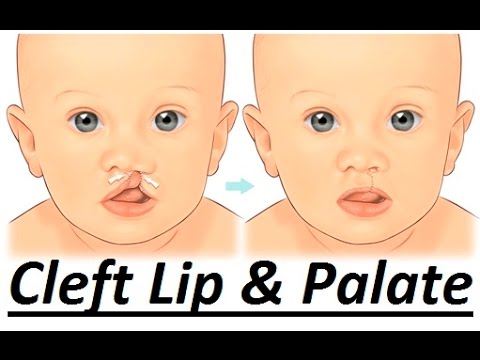 CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011) and the Birth Defects Study To Evaluate Pregnancy exposureS (BD-STEPS; began with births in 2014), to understand the causes of and risks for birth defects, including orofacial clefts.
CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011) and the Birth Defects Study To Evaluate Pregnancy exposureS (BD-STEPS; began with births in 2014), to understand the causes of and risks for birth defects, including orofacial clefts.
Recently, CDC reported on important findings from research studies about some factors that increase the chance of having a baby with an orofacial cleft:
- Smoking―Women who smoke during pregnancy are more likely to have a baby with an orofacial cleft than women who do not smoke.2-3
- Diabetes―Women with diabetes diagnosed before pregnancy have an increased risk of having a child with a cleft lip with or without cleft palate, compared to women who did not have diabetes.5
- Use of certain medicines―Women who used certain medicines to treat epilepsy, such as topiramate or valproic acid, during the first trimester (the first 3 months) of pregnancy have an increased risk of having a baby with cleft lip with or without cleft palate, compared to women who didn’t take these medicines.
 6-7
6-7
CDC continues to study birth defects, such as cleft lip and cleft palate, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.
Diagnosis
Orofacial clefts, especially cleft lip with or without cleft palate, can be diagnosed during pregnancy by a routine ultrasound. They can also be diagnosed after the baby is born, especially cleft palate. However, sometimes certain types of cleft palate (for example, submucous cleft palate and bifid uvula) might not be diagnosed until later in life.
Management and Treatment
Services and treatment for children with orofacial clefts can vary depending on the severity of the cleft; the child’s age and needs; and the presence of associated syndromes or other birth defects, or both.
Surgery to repair a cleft lip usually occurs in the first few months of life and is recommended within the first 12 months of life. Surgery to repair a cleft palate is recommended within the first 18 months of life or earlier if possible.8 Many children will need additional surgical procedures as they get older. Surgical repair can improve the look and appearance of a child’s face and might also improve breathing, hearing, and speech and language development. Children born with orofacial clefts might need other types of treatments and services, such as special dental or orthodontic care or speech therapy.4,8
Surgery to repair a cleft palate is recommended within the first 18 months of life or earlier if possible.8 Many children will need additional surgical procedures as they get older. Surgical repair can improve the look and appearance of a child’s face and might also improve breathing, hearing, and speech and language development. Children born with orofacial clefts might need other types of treatments and services, such as special dental or orthodontic care or speech therapy.4,8
With treatment, most children with orofacial clefts do well and lead a healthy life. Some children with orofacial clefts may have issues with self-esteem if they are concerned with visible differences between themselves and other children. Parent-to-parent support groups can prove to be useful for families of babies with birth defects of the head and face, such as orofacial clefts.
References
- Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A, Alverson CJ, Lupo PJ, Riehle‐Colarusso T, Cho SJ, Aggarwal D, Kirby RS.
 National population‐based estimates for major birth defects, 2010–2014. Birth Defects Research. 2019; 111(18): 1420-1435.
National population‐based estimates for major birth defects, 2010–2014. Birth Defects Research. 2019; 111(18): 1420-1435. - Little J, Cardy A, Munger RG. Tobacco smoking and oral clefts: a meta-analysis. Bull World Health Organ. 2004;82:213-18.
- Honein MA, Rasmussen SA, Reefhuis J, Romitti P, Lammer EJ, Sun L, Correa A. Maternal smoking, environmental tobacco smoke, and the risk of oral clefts. Epidemiology 2007;18:226–33.
- Yazdy MM, Autry AR, Honein MA, Frias JL. Use of special education services by children with orofacial clefts. Birth Defects Research (Part A): Clinical and Molecular Teratology 2008;82:147-54.
- Correa A, Gilboa SM, Besser LM, Botto LD, Moore CA, Hobbs CA, Cleves MA, Riehle-Colarusso TJ, Waller DK, Reece EA. Diabetes mellitus and birth defects. American Journal of Obstetrics and Gynecology 2008;199:237.e1-9.
- Margulis AV, Mitchell AA, Gilboa SM, Werler MM, Glynn RJ, Hernandez-Diaz S, National Birth Defects Prevention Study.
 Use of topiramate in pregnancy and risk of oral clefts. American Journal of Obstetrics and Gynecology 2012;207:405.e1-e7.
Use of topiramate in pregnancy and risk of oral clefts. American Journal of Obstetrics and Gynecology 2012;207:405.e1-e7. - Werler MM, Ahrens KA, Bosco JL, Michell AA, Anderka MT, Gilboa SM, Holmes LB, National Birth Defects Prevention Study. Use of antiepileptic medications in pregnancy in relation to risks of birth defects. Annals of Epidemiology 2011;21:842-50.
- American Cleft Palate-Craniofacial Association. Parameters for evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies. Revised edition, Nov 2009. Chapel Hill, NC. P. 1-34. https://acpa-cpf.org/wp-content/uploads/2017/06/Parameters_Rev_2009_9_.pdf
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.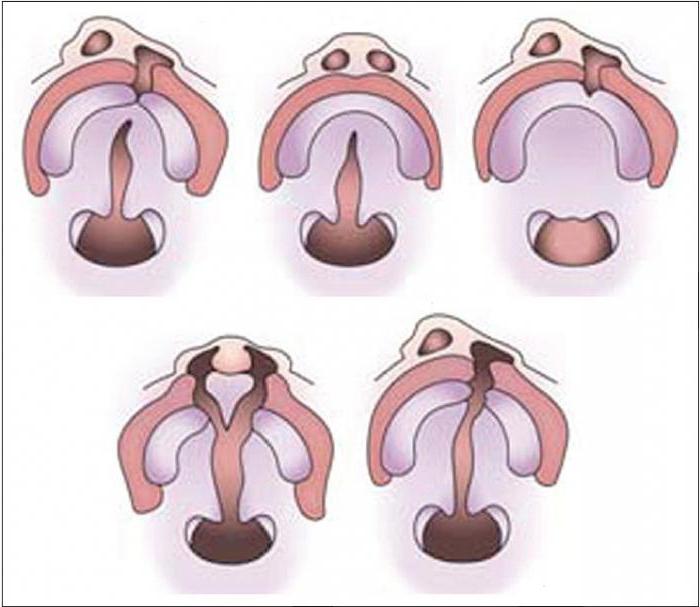
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
Congenital cleft lip and palate — unique results of treatment at the Turner National Research Center for Traumatology and Orthopedics of the Russian Ministry of Health
surgical treatment of congenital cleft lip and palate of all citizens of the Russian Federation. Assistance is provided under the program of state guarantees of free assistance to citizens and within the framework of high-tech medical care. During the work, vast experience has been accumulated, unique methods of leading specialists have been patented. Treatment is carried out on the basis of the Clinic of Maxillofacial and Reconstructive Plastic Surgery.What are congenital cleft lip and palate?
Congenital cleft lip and palate (cheiloschisis) is a splitting of the soft tissues in the middle part of the lip (cleft cleft lip) and/or rupture of the palate (colloquial cleft palate).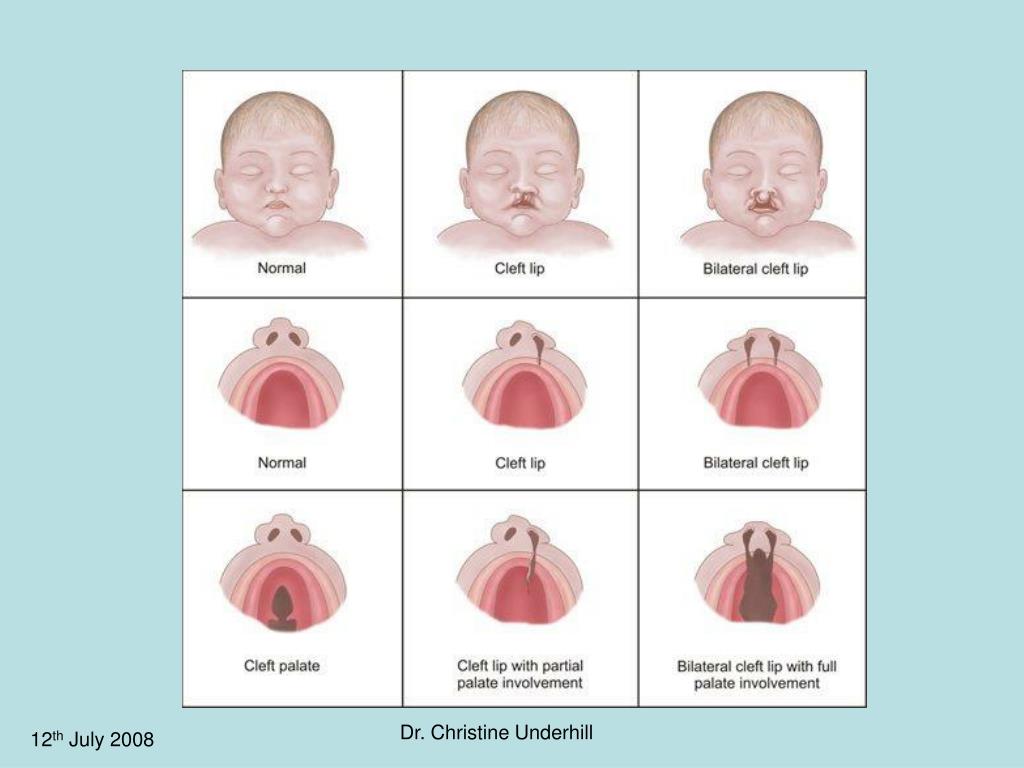 This severe malformation of the maxillofacial region is accompanied by gross functional disorders. In addition, a feature of this pathology is a pronounced deformation of the nose in the form of shortening of the nasal septum, flattening of the tip and wings of the nose. Pathologically attached muscles of the upper lip and nasal region further exacerbate these deformities.
This severe malformation of the maxillofacial region is accompanied by gross functional disorders. In addition, a feature of this pathology is a pronounced deformation of the nose in the form of shortening of the nasal septum, flattening of the tip and wings of the nose. Pathologically attached muscles of the upper lip and nasal region further exacerbate these deformities.
This pathology is formed in the embryo up to 8-12 weeks due to the processes of the palate and lips not fused in time. Congenital cleft lip and palate is more common in boys.
The average birth rate of children with cleft lip and palate is 1:800 newborns. In the most industrially intense regions with a developed chemical industry, the frequency of a child being born with a congenital cleft lip and palate is much higher: 1:500/1:450 newborns.
The process of correction of congenital cleft lip and palate and subsequent stages of rehabilitation is often complicated by a variety of combined pathologies from other organs, in particular the nervous system.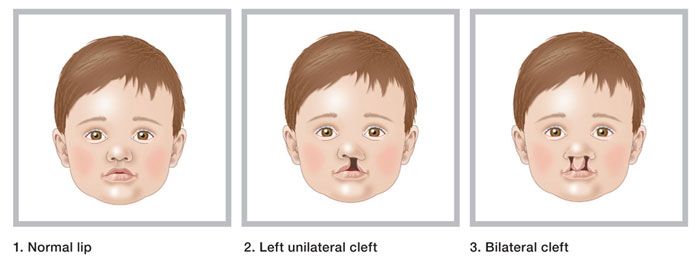 Anatomical changes in the maxillofacial region lead to a persistent functional defect in all departments of voice and speech production. A severe speech disorder develops, rhinolalia, in which all aspects of speech suffer: breathing, voice, changes in the muscles of the pharynx, oral cavity and face are observed, pathological articulation develops, phonemic hearing is disturbed, and auditory perception is distorted. The severity of anatomical and functional disorders is directly related to the type of cleft lip.
Anatomical changes in the maxillofacial region lead to a persistent functional defect in all departments of voice and speech production. A severe speech disorder develops, rhinolalia, in which all aspects of speech suffer: breathing, voice, changes in the muscles of the pharynx, oral cavity and face are observed, pathological articulation develops, phonemic hearing is disturbed, and auditory perception is distorted. The severity of anatomical and functional disorders is directly related to the type of cleft lip.
Children with congenital cleft lip and palate are childhood invalids, and until the end of the formation of the maxillofacial region, up to 14–16 years, as a rule, they are under the constant attention of a surgeon, orthodontist, pediatrician, neuropathologist, speech therapist. However, with a clear, well-coordinated work of highly qualified specialists based on specialized centers, with the active participation and support of parents, it is possible to significantly reduce the period of disability for children.
What is the cause of congenital cleft lip and palate?
“One of the main causes of congenital cleft lip and palate is maternal illness in early pregnancy. This may be the influence of psychogenic factors: severe stress, unrest. This may be work at some enterprises with occupational hazards. Undoubtedly, bad habits cause irreparable harm to the development of the fetus. According to statistics, about 10-15% of the total number of children born with clefts have a genetic predisposition" - informs the head of the Department of Pediatric Maxillofacial and Plastic Surgery (Department 8) of the FSBI "Turner National Research Center for Pediatric Traumatology and Orthopedics" Ministry of Health of Russia, candidate of medical sciences, maxillofacial surgeon Stepanova Yulia Vladimirovna.
Diagnosis and classification
The diagnosis of "congenital cleft lip and palate" is clinical and is established by a doctor on the basis of a visual examination, anthropometric, radiological and ultrasound methods of research.
Types of congenital cleft lip and palate:
- unilateral cleft lip: hidden, partial, complete;
- bilateral cleft lip: hidden, partial, complete;
- unilateral cleft lip and alveolar process: partial, complete;
- bilateral cleft lip and alveolar process: partial, complete;
- unilateral complete cleft lip and palate;
- Bilateral complete cleft lip and palate
- congenital cleft palate: submucosal, partial, complete.
Cleft lip and palate treatment - unique techniques and inspiring results
At the Turner National Research Center for Pediatric Traumatology and Orthopedics of the Ministry of Health of Russia, complex treatment of children with cleft lip and palate is carried out by highly qualified specialists. For successful treatment of cleft lip and palate, it is necessary to predict the expected results and a clear plan for the various stages. From the birth of a child to the age of 14-16, a multi-stage treatment is carried out with the participation of a large number of specialists.
Treatment of children with this pathology includes:
- preoperative orthodontic and orthopedic preparation;
- surgical treatment (reconstructive and plastic surgery): must be completed before the child's speech - by 3 years;
- orthodontic and orthopedic treatment after surgery, preventing the development of secondary deformities of the nose and upper lip.
The entire period of complex treatment can be conditionally divided into 5 stages:
- Early orthodontic treatment: from birth to cheilorhinoplasty. The duration of this stage depends on the type and severity of the cleft and the general somatic condition of the patient. This stage can last up to 3-6 months, and in the presence of severe concomitant defects - up to 12-18 months. The coordinator of the work is the surgeon.
- Cheilorhinoplasty is a complex plastic surgery, in which the task is not only to restore the anatomical shape of the upper lip and palate, but also to normalize the functions of breathing, nutrition and speech.
 When performing the primary operation, the task is not only to eliminate the congenital cleft of the upper lip, to create the correct shape of the red border, but also to correct the congenital deformity of the nose in full, create a sufficient depth of the vestibule of the mouth, and perform primary periosteoplasty.
When performing the primary operation, the task is not only to eliminate the congenital cleft of the upper lip, to create the correct shape of the red border, but also to correct the congenital deformity of the nose in full, create a sufficient depth of the vestibule of the mouth, and perform primary periosteoplasty. - Postoperative observation, elimination of residual deformities, preparation for uranoplasty. A huge role in maintaining the optimal result and consolidating the success obtained during the primary surgical intervention is played by massage, myogymnastics of the lips and nose, as well as the use of individual inserts in the nasal passages in the postoperative period, which allow you to save nasal breathing, keep the nasal septum and wing in the correct position, prevent rough scarring. The correction of the liner is carried out taking into account the growth of the child - 1 time in 3 months. The duration of use of the inserts is determined taking into account the individual characteristics of each patient.
 These measures not only prevent the development of cicatricial deformities, but also contribute to the growth and development of underdeveloped tissues at birth. Both a doctor and parents can carry out these conservative procedures at home under the constant periodic supervision of a surgeon and a speech therapist. Orthodontic treatment prior to uranoplasty is combined with the use of a floating obturator. This medical device significantly improves the functions of nutrition, swallowing, and subsequently speech, prevents the formation of a pathological position of the tongue in the oral cavity and distorted compensatory sound production, contributes to the normalization of impaired respiratory function and aerodynamic conditions of sound production, and allows speech therapy work in the preoperative period. The better the early orthodontic treatment, the more effective the results of subsequent speech correction, and hence social rehabilitation. Preparation for uranoplasty lasts exactly as long as it takes to normalize the bite.
These measures not only prevent the development of cicatricial deformities, but also contribute to the growth and development of underdeveloped tissues at birth. Both a doctor and parents can carry out these conservative procedures at home under the constant periodic supervision of a surgeon and a speech therapist. Orthodontic treatment prior to uranoplasty is combined with the use of a floating obturator. This medical device significantly improves the functions of nutrition, swallowing, and subsequently speech, prevents the formation of a pathological position of the tongue in the oral cavity and distorted compensatory sound production, contributes to the normalization of impaired respiratory function and aerodynamic conditions of sound production, and allows speech therapy work in the preoperative period. The better the early orthodontic treatment, the more effective the results of subsequent speech correction, and hence social rehabilitation. Preparation for uranoplasty lasts exactly as long as it takes to normalize the bite. Orientation sessions are held with a speech therapist. Constant monitoring by the surgeon and all the necessary specialists is carried out.
Orientation sessions are held with a speech therapist. Constant monitoring by the surgeon and all the necessary specialists is carried out. - Uranoplasty – the G. I. Turner National Research Center for Pediatric Traumatology and Orthopedics of the Ministry of Health of Russia uses a sparing uranoplasty technique, which allows in one stage to form an anatomically correct, functionally complete palate in the treatment of any form of cleft. The technique has a patent of the Russian Federation for the invention. Uranoplasty is performed at the age of 8 months to 3 years, depending on the form of the cleft and the somatic condition of the child.
- Final rehabilitation: adherence to the basic principles of rehabilitation of children with congenital cleft lip and palate not only significantly improves the aesthetic and functional results of treatment, but also minimizes the number of repeated corrective operations. The stage of final rehabilitation includes activities for the production of sounds and speech formation.
 One of the main indicators of the effectiveness of surgical treatment of children with congenital cleft lip and palate is the quality of speech development in the postoperative period. Children with congenital cleft palate begin classes with a speech therapist in the hospital from the first days after uranoplasty. In addition, during this period, an orthodontist actively monitors the state of bite. All possible deviations in the development of the upper jaw, the position of the intermaxillary bone with bilateral cleft lip, anomalies in the position and eruption of teeth are revealed. The choice of apparatus and the tasks of orthodontic treatment are determined by the specific manifestations of the anomaly and the age of the patient. During the period of temporary occlusion, removable single-jaw and double-jaw devices are used.
One of the main indicators of the effectiveness of surgical treatment of children with congenital cleft lip and palate is the quality of speech development in the postoperative period. Children with congenital cleft palate begin classes with a speech therapist in the hospital from the first days after uranoplasty. In addition, during this period, an orthodontist actively monitors the state of bite. All possible deviations in the development of the upper jaw, the position of the intermaxillary bone with bilateral cleft lip, anomalies in the position and eruption of teeth are revealed. The choice of apparatus and the tasks of orthodontic treatment are determined by the specific manifestations of the anomaly and the age of the patient. During the period of temporary occlusion, removable single-jaw and double-jaw devices are used.
Undoubtedly, the priority of surgical operations in the complex of measures in the treatment of congenital cleft lip and palate. However, this is only one link out of many links in the complex of ongoing activities.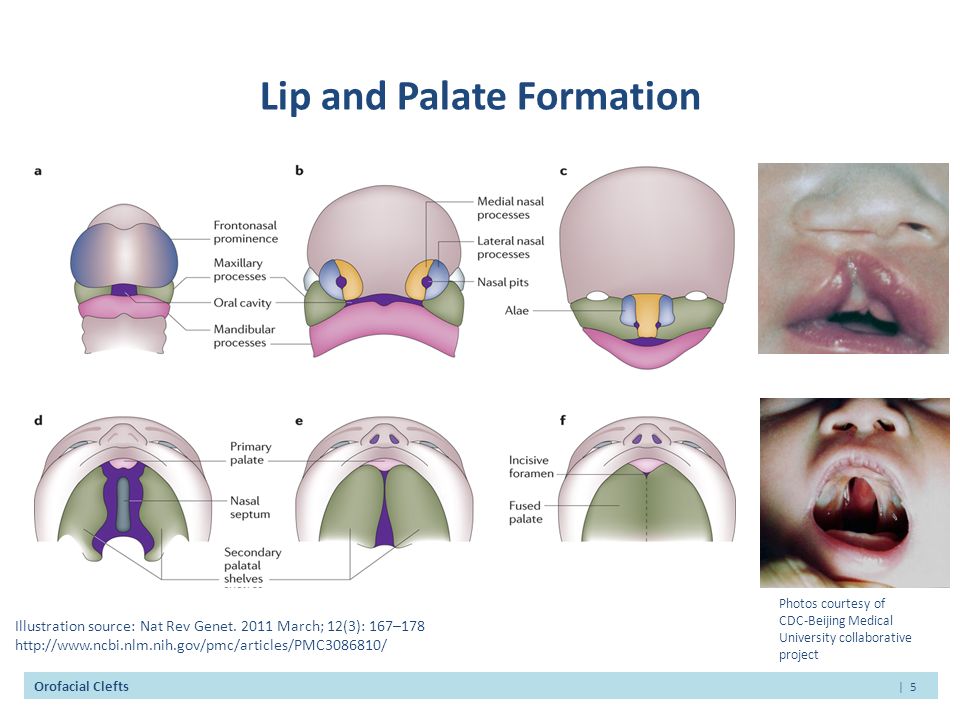 If during the period of preparation for the primary operation of cheilorhinoplasty orthodontic treatment is not carried out, the congenital deformity of the upper jaw is not corrected, then the result of surgical treatment will never be positive, especially in the case of unilateral and bilateral complete cleft lip. The same relationship exists during uranoplasty. Thus, underestimation of the role of orthodontic treatment leads to severe hard-to-remove deformities of the nose, upper lip and upper jaw. This is the main cause of residual and postoperative deformities.
If during the period of preparation for the primary operation of cheilorhinoplasty orthodontic treatment is not carried out, the congenital deformity of the upper jaw is not corrected, then the result of surgical treatment will never be positive, especially in the case of unilateral and bilateral complete cleft lip. The same relationship exists during uranoplasty. Thus, underestimation of the role of orthodontic treatment leads to severe hard-to-remove deformities of the nose, upper lip and upper jaw. This is the main cause of residual and postoperative deformities.
In the majority of patients with congenital cleft lip and palate (up to 70%) of the Turner National Research Center for Traumatology and Orthopedics of the Ministry of Health of Russia, who underwent early speech therapy, early orthodontic treatment, after uranoplasty surgery at the age of up to 3 years, speech develops without nasalization. In 60% of cases, the speech of children after uranoplasty is restored spontaneously, in the remaining patients, the effectiveness of rehabilitation speech therapy techniques increases in the postoperative period.
Results of treatment at the NMB “NMIC of Pediatric Traumatology and Orthopedics named after G. I. Tourner” of the Ministry of Health of Russia
90,000 archaeologists found the remains of a guy with a wolf's mouth and a hare gibe 9000 9000 Archel in Slovakia, the remains of two individuals who were buried in the 17th or 18th century in a storage pit and in a hastily dug grave. One of them belonged to a young man who had orofacial clefts - a cleft palate and a cleft lip. According to scientists, their death could have been violent, since people with similar defects in some societies were considered vampires. This is reported in an article published in the magazine Archaeological and Anthropological Sciences .
Today, one of the most common craniofacial malformations is orofacial clefts, which occur approximately 1. 4 times per thousand newborns. Physicians distinguish three main forms of this congenital malformation: cleft lip (cheiloschis), lip and palate (cheilognatopalatoschis), or only the palate (palatoschis). In colloquial speech, the concepts of cleft lip and cleft palate are used to describe such pathologies. Both genetic and environmental factors are involved in the pathogenesis of this disease.
4 times per thousand newborns. Physicians distinguish three main forms of this congenital malformation: cleft lip (cheiloschis), lip and palate (cheilognatopalatoschis), or only the palate (palatoschis). In colloquial speech, the concepts of cleft lip and cleft palate are used to describe such pathologies. Both genetic and environmental factors are involved in the pathogenesis of this disease.
Although orofacial clefts are fairly common today, human remains with these malformations are rare in an archaeological context. The most famous exception is Pharaoh Tutankhamun, whose tomb was discovered in the Valley of the Kings in 1922. In addition to the cleft palate, paleopathologists diagnosed him with clubfoot, Koehler's disease and some other diseases and injuries. In total, archaeologists know about 50 such examples, and in 80 percent of cases, orofacial clefts were found in adults. So, the remains of one of the individuals were found in Altai, during excavations of the burial of the Andronovo (Fedorovo) culture in the burial ground of Firsovo-XIV. He was a young male aged 18–23 who died about 1883–1665 BC.
He was a young male aged 18–23 who died about 1883–1665 BC.
Silvia Bodorikova from Comenius University, together with colleagues from Australia, Slovakia and France, examined the remains of two people that were discovered during construction work in the city of Dunajska Streda. They were at the bottom of a storage pit (or a hastily dug grave pit) and were covered with soil, which also contained bricks and fragments of pottery. The position of the skeletons, according to archaeologists, indicates that they were buried at the same time.
The remains of an adult were located in a supine position with legs thrown over. They belonged to a man about 173.3 ± 4.8 centimeters tall, who died at the age of 40 to 50 years. Examination of the skull bones showed that he suffered from periodontitis and sinusitis. In addition, one of the vertebrae contained evidence of a healed fracture. Traces of spondylosis were observed on all lumbar vertebrae. Scientists did not find any other serious pathologies or traumatic injuries.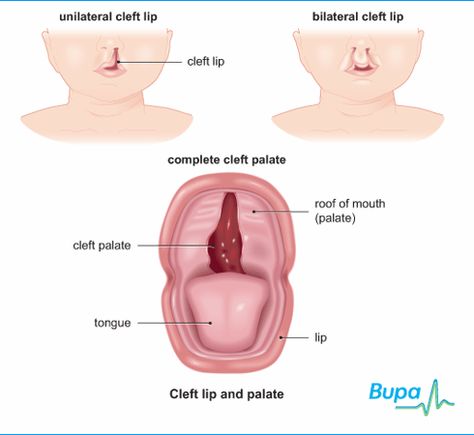
The remains of the second individual belonged to a young man, about 165.6 ± 4.9 centimeters tall, who was buried in a crouched position directly under the body of an adult. Scientists have suggested that he is about 16-18 years old. However, this guy had congenital malformations of the face and dentition - orofacial cleft lip and palate, and this may underestimate the age. In addition, this young man had extra teeth, as well as a number of other pathologies, such as enamel hypoplasia and caries.
Scientists have read the DNA of these people and found that they were not relatives either maternal or paternal. Although the discovered haplogroups are distributed throughout Europe, they are most often found in Western European populations, for example, in Great Britain, Ireland and France. An analysis of stable isotopes of nitrogen and carbon showed that the diet of both people in the last years of their lives consisted largely of animal protein. And radiocarbon analysis indicated that people died in the middle of the 17th - the end of the 18th century.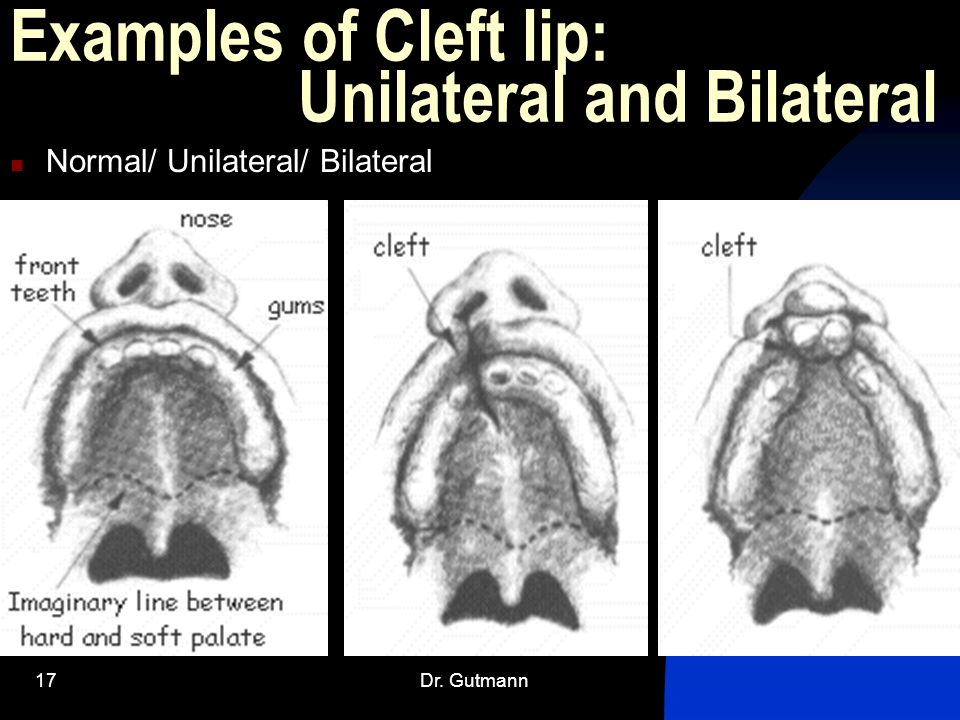
Scientists noted that the remains of a young man with a cleft lip and palate were found in Slovakia for the first time in an archaeological context. Archaeologists reported that in modern populations, such a pathology is much more common. Perhaps this is due to the fact that in the past there was a high mortality of children with orofacial clefts, there were infanticides. In addition, maternal diet may have reduced the incidence of this malformation.
The researchers concluded that both of these people could be foreigners. It seems that the body of a young man was lowered into the pit with his feet down, and, perhaps, he was previously tied up. An adult man was lowered with his head or back down. The bricks present in the backfill, according to archaeologists, could be due to the fact that the buried were considered "dangerous dead". Although the scientists did not find any traumatic injuries, they did not rule out violent death. But, perhaps, they could die from illness, hypothermia, or from some other reason.