Age and weight charts for babies
Growth Charts - Clinical Growth Charts
The clinical growth charts reflect modifications in the format of the individual charts, whereby two individual charts appear on a single page, and data entry tables have been added. The clinical charts have the grids scaled to metric units (kg, cm), with English units (lb, in) as the secondary scale. Clinical charts are available for boys and for girls. The available clinical charts include the following:
Infants, birth to 36 months:
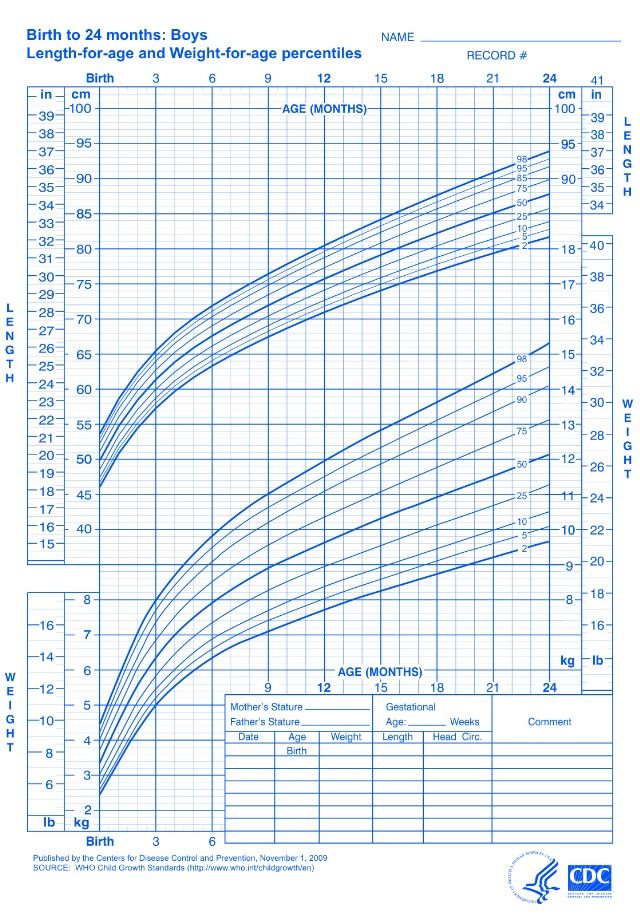
- Length-for-age and Weight-for-age
- Head circumference-for-age and Weight-for-length
Children and adolescents, 2 to 20 years
- Stature-for-age and Weight-for-age
- BMI-for-age
Preschoolers, 2 to 5 years
- Weight-for-stature
The clinical charts for infants and older children were published in two sets.
- Set 1 contains 10 charts (5 for boys and 5 for girls), with the 5th, 10th, 25th, 50th, 75th, 90th, and 95th smoothed percentile lines for all charts, and the 85th percentile for BMI-for-age and weight-for-stature.
- Set 2 contains 10 charts (5 for boys and 5 for girls), with the 3rd, 10th, 25th, 50th, 75th, 90th, and 97th smoothed percentile lines for all charts, and the 85th percentile for BMI-for-age and weight-for-stature.
Set 1 has the outer limits of the curves at the 5th and 95th percentiles. These are the charts that most users in the United States will find useful for the majority of routine clinical assessments. Set 2 has the outer limits of the curves at the 3rd and 97th percentiles for selected applications. Pediatric endocrinologists and others who assess the growth of children with special health care requirements may wish to use the format in set 2 for selected applications.
Two summary files, each with all 10 clinical charts in set 1 or set 2 are also available. These summary files contain the clinical charts from either set 1 or set 2 as described above.
Infants (birth to 24 months) must be measured for length, and the sex appropriate length-for-age or weight-for-length charts for infants, birth to 36 months must be used to plot the measurements. At age 24 months and older, if children can stand unassisted and follow directions, stature should be measured and plotted on the stature-for-age chart for children (2 to 20 years). Otherwise, between 24 and 36 months, length can be used in place of stature.
At age 24 months and older, if children can stand unassisted and follow directions, stature should be measured and plotted on the stature-for-age chart for children (2 to 20 years). Otherwise, between 24 and 36 months, length can be used in place of stature.
BMI-for-age charts are recommended to assess weight in relation to stature for children ages 2 to 20 years. The weight-for-stature charts are available as an alternative to accommodate children ages 2-5 years who are not evaluated beyond the preschool years. However, all health care providers should consider using the BMI-for-age charts to be consistent with current recommendations.
All individual 2000 CDC growth charts have an initial publication date of May 30, 2000. For various reasons, modifications were made to charts after the initial publication date. For example, the individual charts were modified to create the clinical charts, which were made available on October 16, 2000. Subsequent modifications were made to selected clinical charts to correct or enhance particular aspects of the scales on the graphs. In all cases, the data points in the corresponding data file for each modified chart remain unchanged from the initial release on May 30, 2000. Where applicable, when selected clinical charts were further modified, the date is indicated on each chart. The clinical growth charts for stature-for-age were modified because the scale for inches was not correctly aligned with the metric scale. The clinical growth charts for infant length-for-age and infant weight-for-age were revised to improve the appearance of the scale for inches on the length charts by extending the indicators at ½ inch increments, and enhancing alignment of the English with the metric scales on both the length and weight scales.
In all cases, the data points in the corresponding data file for each modified chart remain unchanged from the initial release on May 30, 2000. Where applicable, when selected clinical charts were further modified, the date is indicated on each chart. The clinical growth charts for stature-for-age were modified because the scale for inches was not correctly aligned with the metric scale. The clinical growth charts for infant length-for-age and infant weight-for-age were revised to improve the appearance of the scale for inches on the length charts by extending the indicators at ½ inch increments, and enhancing alignment of the English with the metric scales on both the length and weight scales.
Users should use the most recent version of each chart, as available on the growth charts web site.
To view, print, and reproduce clinical growth charts
All clinical growth charts may be viewed, downloaded, and printed in Adobe Acrobat. For routine viewing on a computer monitor and printing on a laser printer, the individual charts are available as PDF files (Black and White). All clinical charts have been colorized for viewing and printing. When routed to a color printer, the clinical charts for boys will print in blue and the clinical charts for girls will print in red. Otherwise, these same charts can be routed to a black-and-white printer, and will print in black-and-white. Higher resolution PDF files (Color) are available to provide the highest resolution and are intended to be used as a high quality print master for quantity production when using the services of a commercial printing facility. The recommended ink colors for printing are Pantone 206 red (for girls) and Pantone 286 blue (for boys). The recommended paper weight is 80#. Charts should be printed as two-sided copies, in the following combinations for each sex:
All clinical charts have been colorized for viewing and printing. When routed to a color printer, the clinical charts for boys will print in blue and the clinical charts for girls will print in red. Otherwise, these same charts can be routed to a black-and-white printer, and will print in black-and-white. Higher resolution PDF files (Color) are available to provide the highest resolution and are intended to be used as a high quality print master for quantity production when using the services of a commercial printing facility. The recommended ink colors for printing are Pantone 206 red (for girls) and Pantone 286 blue (for boys). The recommended paper weight is 80#. Charts should be printed as two-sided copies, in the following combinations for each sex:
Infants, birth to 36 months:
- Side 1: Length for age + Weight-for-age
- Side 2: Head circumference-for-age + Weight-for-length
Children and adolescents, 2 to 20 years:
- Side 1: Stature-for-age + Weight-for-length
- Side 2: BMI-for-age or
- Weight-for-stature (age 2 to 5 years only)
Set 1: Clinical charts with 5th and 95th percentiles
Birth to 36 months (5th-95th percentile)
Boys Length-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 41 KB] Modified 4/20/01
Color Cdc-pdf[PDF – 44 KB] Modified 4/20/01
Spanish Version, Color Cdc-pdf[PDF – 44 KB] Modified 4/20/01
French Version, Color Cdc-pdf[PDF – 44 KB] Modified 4/20/01
B&W Press-Ready Cdc-pdf[PDF – 186 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 200 KB] Modified 9/15/05
Data table of Length-for-age charts
Data table of Weight-for-age charts
Boys Head circumference-for-age and Weight-for-length
B&W Cdc-pdf[PDF – 48 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 48 KB] Modified 10/16/00
Spanish Version Color Cdc-pdf[PDF – 52 KB] Modified 10/16/00
French Version Color Cdc-pdf[PDF – 56 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 206 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 236 KB] Modified 9/15/05
Data table of Head circumference-for-age charts
Data table of Weight-for-length charts
Girls Length-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 40 KB] Modified 4/20/01
Color Cdc-pdf[PDF – 40 KB] Modified 4/20/01
Spanish Version, Color Cdc-pdf[PDF – 50 KB] Modified 4/20/01
French Version, Color Cdc-pdf[PDF – 44 KB] Modified 4/20/01
B&W Press-Ready Cdc-pdf[PDF – 186 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 401 KB] Modified 9/15/05
Data table of Length-for-age charts
Data table of Weight-for-age charts
Girls Head circumference-for-age and Weight-for-length
B&W Cdc-pdf[PDF – 48 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 55 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 60 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 55 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 206 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 440 KB] Modified 9/15/05
Data table of Head circumference-for-age charts
Data table of Weight-for-length charts
Children 2 to 20 years (5th-95th percentile)
Boys Stature-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 77 KB] Modified 11/21/00
Color Cdc-pdf[PDF – 77 KB] Modified 11/21/00
Spanish Version, Color Cdc-pdf[PDF – 63 KB] Modified 11/21/00
French Version, Color Cdc-pdf[PDF – 78 KB] Modified 11/21/00
B&W Press-Ready Cdc-pdf[PDF – 208 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 260 KB] Modified 9/15/05
Data table of Stature-for-age charts
Data table of Weight-for-age charts
Boys BMI-for-age
B&W Cdc-pdf[PDF – 61 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 61 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 50 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 64 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 141 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 183 KB] Modified 9/15/05
Data table of BMI-for-age charts
Girls Stature-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 77 KB] Modified 11/21/00
Color Cdc-pdf[PDF – 77 KB] Modified 11/21/00
Spanish Version, Color Cdc-pdf[PDF – 62 KB] Modified 11/21/00
French Version, Color Cdc-pdf[PDF – 79 KB] Modified 11/21/00
B&W Press-Ready Cdc-pdf[PDF – 208 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 499 KB] Modified 9/15/05
Data table of Stature-for-age charts
Data table of Weight-for-age charts
Girls BMI-for-age
B&W Cdc-pdf[PDF – 67 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 61 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 51 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 64 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 142 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 339 KB] Modified 9/15/05
Data table of BMI-for-age charts
Optional Chart (5th-95th percentile)
Boys Weight-for-stature
B&W Cdc-pdf[PDF – 40 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 41 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 148 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 180 KB] Modified 9/15/05
Data table of Weight-for-stature charts
Girls Weight-for-stature
B&W Cdc-pdf[PDF – 40 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 41 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 147 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 334 KB] Modified 9/15/05
Data table of Weight-for-stature charts
Set 2: Clinical charts with 3rd and 97th percentiles
Birth to 36 months (3rd -97th percentile)
Boys Length-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 41 KB] Modified 4/20/01
Color Cdc-pdf[PDF – 47 KB] Modified 4/20/01
Spanish Version, Color Cdc-pdf[PDF – 47 KB] Modified 4/20/01
French Version, Color Cdc-pdf[PDF – 44 KB] Modified 4/20/01
B&W Press-Ready Cdc-pdf[PDF – 186 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 201 KB] Modified 9/15/05
Data table of Length-for-age charts
Data table of Weight-for-age charts
Boys Head circumference-for-age and Weight-for-length
B&W Cdc-pdf[PDF – 48 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 52 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 53 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 51 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 207 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 223 KB] Modified 9/15/05
Data table of Head circumference-for-age charts
Data table of Weight-for-length charts
Girls Length-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 41 KB] Modified 4/20/01
Color Cdc-pdf[PDF – 48 KB] Modified 4/20/01
Spanish Version, Color Cdc-pdf[PDF – 48 KB] Modified 4/20/01
French Version, Color Cdc-pdf[PDF – 45 KB] Modified 4/20/01
B&W Press-Ready Cdc-pdf[PDF – 186 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 390 KB] Modified 9/15/05
Data table of Length-for-age charts
Data table of Weight-for-age charts
Girls Head circumference-for-age and Weight-for-length
B&W Cdc-pdf[PDF – 48 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 53 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 54 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 52 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 206 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 434 KB] Modified 9/15/05
Data table of Head circumference-for-age charts
Data table of Weight-for-length charts
Children 2 to 20 years (3rd-97th percentile)
Boys Stature-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 79 KB] Modified 11/21/00
Color Cdc-pdf[PDF – 83 KB] Modified 11/21/00
Spanish Version, Color Cdc-pdf[PDF – 61 KB] Modified 11/21/00
French Version, Color Cdc-pdf[PDF – 79 KB] Modified 11/21/00
B&W Press-Ready Cdc-pdf[PDF – 208 KB] Modified 9/15/05
Color Press-ready Cdc-pdf[PDF – 250 KB] Modified 9/15/05
Data table of Stature-for-age charts
Data table of Weight-for-age charts
Boys BMI-for-age
B&W Cdc-pdf[PDF – 64 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 68 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 52 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 66 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 153 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 173 KB] Modified 9/15/05
Data table of BMI-for-age charts
Girls Stature-for-age and Weight-for-age
B&W Cdc-pdf[PDF – 79 KB] Modified 11/21/00
Color Cdc-pdf[PDF – 84 KB] Modified 11/21/00
Spanish Version, Color Cdc-pdf[PDF – 62 KB] Modified 11/21/00
French Version, Color Cdc-pdf[PDF – 81 KB] Modified 11/21/00
B&W Press-Ready Cdc-pdf[PDF – 218 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 488 KB] Modified 9/15/05
Data table of Stature-for-age charts
Data table of Weight-for-age charts
Girls BMI-for-age
B&W Cdc-pdf[PDF – 54 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 58 KB] Modified 10/16/00
Spanish Version, Color Cdc-pdf[PDF – 52 KB] Modified 10/16/00
French Version, Color Cdc-pdf[PDF – 67 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 152 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 334 KB] Modified 9/15/05
Data table of BMI-for-age charts
Optional Chart (3rd-97th percentile)
Boys Weight-for-stature
B&W Cdc-pdf[PDF – 31 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 34 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 158 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 168 KB] Modified 9/15/05
Data table of Weight-for-stature charts
Girls Weight-for-stature
B&W Cdc-pdf[PDF – 40 KB] Modified 10/16/00
Color Cdc-pdf[PDF – 46 KB] Modified 10/16/00
B&W Press-Ready Cdc-pdf[PDF – 157 KB] Modified 9/15/05
Color Press-Ready Cdc-pdf[PDF – 323 KB] Modified 9/15/05
Data table of Weight-for-stature charts
Summary files
Set 1 summary file; 5th, 10th, 25th, 50th, 75th, 90th, 95th percentiles
Download all 10 charts in Set 1
B&W Cdc-pdf[PDF – 409K]
Color Cdc-pdf[PDF – 418 KB]
Set 2 summary file; 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles
Download all 10 charts in Set 2
B&W Cdc-pdf[PDF – 408K]
Color Cdc-pdf[PDF – 423 KB]
Growth Charts - Background
Introduction
The growth charts consist of a series of percentile curves that illustrate the distribution of selected body measurements in U. S. children. Pediatric growth charts have been used by pediatricians, nurses, and parents to track the growth of infants, children, and adolescents in the United States since 1977. The 1977 growth charts were developed by the National Center for Health Statistics (NCHS) as a clinical tool for health professionals to determine if the growth of a child is adequate. The 1977 charts were also adopted by the World Health Organization for international use.
S. children. Pediatric growth charts have been used by pediatricians, nurses, and parents to track the growth of infants, children, and adolescents in the United States since 1977. The 1977 growth charts were developed by the National Center for Health Statistics (NCHS) as a clinical tool for health professionals to determine if the growth of a child is adequate. The 1977 charts were also adopted by the World Health Organization for international use.
When the 1977 NCHS growth charts were first developed, NCHS recommended that they be revised periodically as necessary. With more recent and comprehensive national data now available, along with improved statistical procedures, the 1977 growth charts were revised and updated to make them a more valuable clinical tool for health professionals. The 2000 CDC growth charts represent the revised version of the 1977 NCHS growth charts. Most of the data used to construct these charts come from the National Health and Nutrition Examination Survey (NHANES), which has periodically collected height and weight and other health information on the American population since the early 1960’s.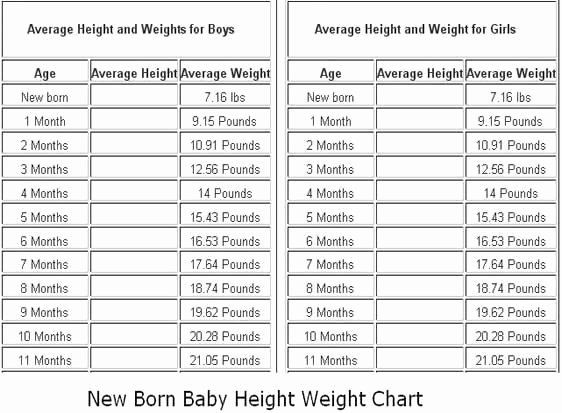
Growth charts are not intended to be used as a sole diagnostic instrument. Instead, growth charts are tools that contribute to forming an overall clinical impression for the child being measured. The revised growth charts provide an improved tool for evaluating the growth of children in clinical and research settings.
The 2000 CDC Growth Charts and the New BMI-For-Age Charts
The revised growth charts consist of 16 charts (8 for boys and 8 for girls). These charts represent revisions to the 14 previous charts, as well as the introduction of two new body mass index-for-age (BMI-for-age) charts for boys and for girls, ages 2 to 20 years.
Most of the specific differences between the revised charts and the original charts occur in the charts for infants, where national data were previously lacking. The revised head circumference charts also show some noticeable differences when compared to the earlier charts. Compared to the original infant charts that were based on primarily formula-fed infants, the revised growth charts for infants contain a better mix of both breast- and formula-fed infants in the U. S. population. (On average, since 1970 approximately one-half of children born in the United States are reported to have been breast fed at some point, and about one-third have been breast fed for 3 months or more.) The addition of the BMI charts is probably the single most significant new feature of the revised growth charts.
S. population. (On average, since 1970 approximately one-half of children born in the United States are reported to have been breast fed at some point, and about one-third have been breast fed for 3 months or more.) The addition of the BMI charts is probably the single most significant new feature of the revised growth charts.
These BMI-for-age charts were created for use in place of the 1977 weight-for-stature charts. BMI (wt/ht2) is calculated from weight and height measurements and is used to judge whether an individual’s weight is appropriate for their height. BMI is the most commonly used approach to determine if adults are overweight or obese and is also the recommended measure to determine if children are overweight. The new BMI growth charts can be used clinically beginning at 2 years of age, when an accurate stature can be obtained.
In recent years, BMI has received increased attention for pediatric use. In 1994, an expert committee charged with developing guidelines for overweight in adolescent preventive services (ages 11-21 years) recommended that BMI be used routinely to screen for overweight adolescents.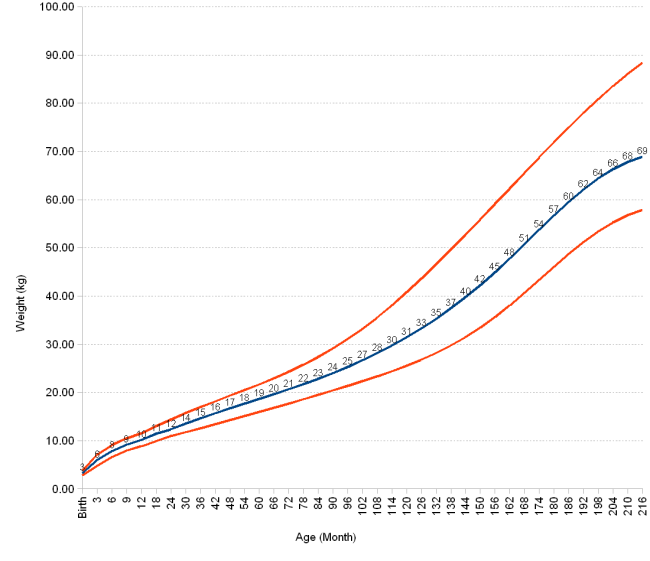 In addition, in 1997 an expert committee on the assessment and treatment of childhood obesity concluded that BMI should be used to screen for overweight children, ages 2 years and older, using the BMI curves from the revised growth charts. BMI can also be used to characterize underweight (though no expert guidelines exist for the classification of underweight based on BMI).
In addition, in 1997 an expert committee on the assessment and treatment of childhood obesity concluded that BMI should be used to screen for overweight children, ages 2 years and older, using the BMI curves from the revised growth charts. BMI can also be used to characterize underweight (though no expert guidelines exist for the classification of underweight based on BMI).
Methods and Development
For more information about the methods and development of the CDC Growth Charts, please see the 2000 CDC Growth Charts for the United States: Methods and Development Cdc-pdf[PDF – 5M] report.
Tables of weight and height of the child by months and by years. For boys and for girls.
The height and weight of a child are the main indicators of his physical development. That is why immediately after the birth of the baby, it is imperative to measure the weight of his body and the length of the body and continue to weigh himself daily at the same time until discharge from the hospital.
There are many factors that affect the physical development of a child, for example:0010
How to understand what is the norm?
The All-Russian Health Organization recommended special tables for matching the height and weight of children, or as they are called, centile tables. At each examination, the pediatrician measures the height and weight of the child, compares the obtained values \u200b\u200bwith the standard indicators. Such tables allow you to identify obvious pathologies, for a more accurate analysis, the doctor calculates additional indicators using special formulas.
Monthly infant weight and height chart (up to 1 year)
The table shows the average height and weight of infants (under 1 year of age) by month for boys and girls.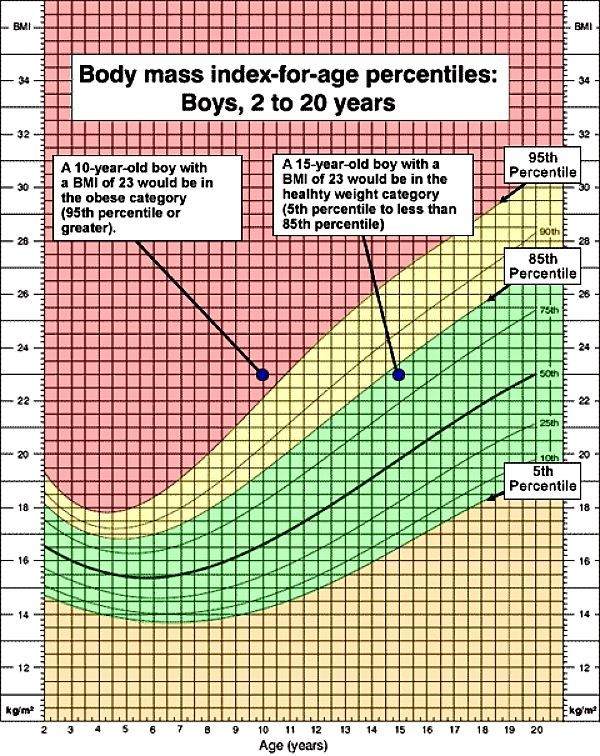
| Age | Girls | Boys | ||||||
| , kg | 9000 9000, KG, KG | 9000 9000, KG, KG 9000 9000, KG, KG 9,000|||||||
| Newborns | 3.33 ± 0.44 | 49.50 ± 1.63 | 3.53 ± 0.45 | 50.43 ± 1.89 | 1 month | 4.15 ± 0.54 | 53.51 ± 2.13 | 4.32 ± 0.64 | 54.53 ± 2.32 |
| 2 months | 5.01 ± 0.56 | 56.95 ± 2.18 | 5 .29 ± 0.76 | 57.71 ± 2.48 | ||||
| 3 months | 6.07 ± 0.58 | 60.29 ± 2.08 903 | 61.30 ± 2.41 | |||||
| 4 months | 6.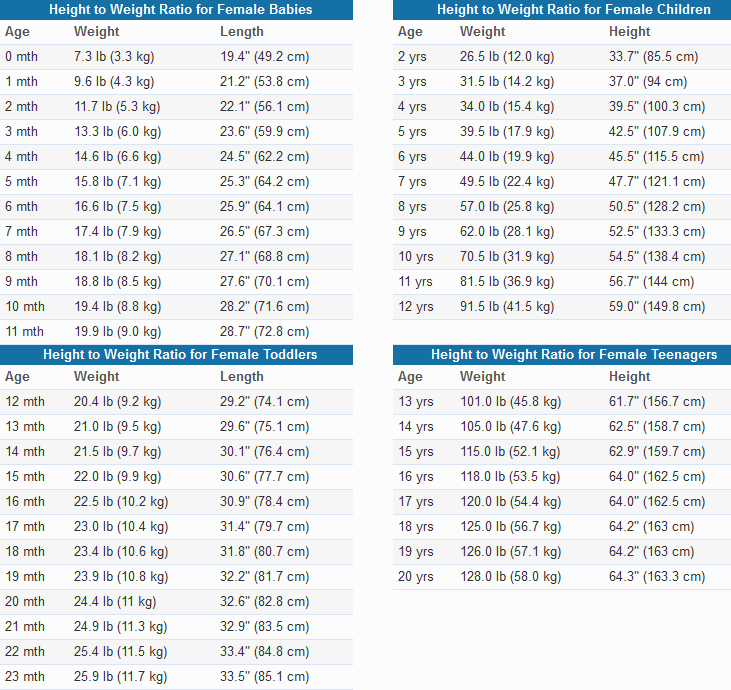 55 ± 0.79 55 ± 0.79 | 62.15 ± 2.49 | 6.87 ± 0.74 | 63.79 ± 2.68 | ||||
| 9000 3 months | 7.38 ± 0.96 | 63.98 ± 2.49 | 7.82 ± 0.80 | 66.92 ± 1.99 | ||||
| 6 months | 7.97 ± 0.92 | 66.60 ± 2.44 | 8.77 ± 0.78 | 67.995 ± 2.24 80049 7 months | 8.25 ± 0.95 | 67.44 ± 2.64 | 8.92 ± 1.11 | 69.56 ± 2.61 |
| 9000 3 months 9000 | 8.35 ± 1.10 | 69.84 ± 2.07 | 9.46 ± 0.98 | 71.17 ± 2.24 | ||||
| 9000 9 months | 9.28 ± 1 .01 | 70.69 ± 2.21 | 9.89 ± 1.18 | 72.84 ± 2.71 | ||||
| 10 months | 9.52 ± 1.3572.11 ± 2.86 | 10.35 ± 1.12 | 73.91 ± 2.65 | |||||
| 11 months | 9.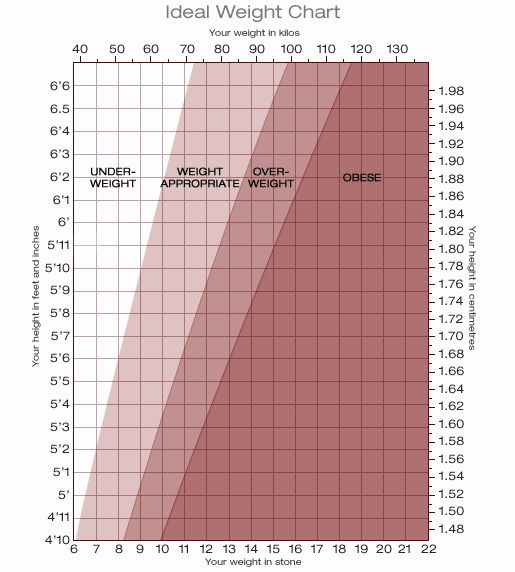 80 ± 0, 0, 80 80 ± 0, 0, 80 | 73.60 ± 2.73 | 10.47 ± 0.98 | 74.90 ± 2.55 | ||||
| 10.04 ± 1.16 | 74.78 ± 2.54 | 10.66 ± 1.21 | 75.78 ± 2.79 | |||||
Table of weight and height of the child by years (from 1 to 18 years)
weight of the child by years aged 1 to 18 years for boys and girls.
| Age | Girls | Boys | |||||
| , kg | 9000 9000, KG, KG | 9000 9000, KG, KG 9000 9000, KG, KG||||||
| 1 year 3 months | 10.52 ± 1.27 | 76.97 ± 3.00 | 11.40 ± 1.30 | 79.45 ± 3.56 | |||
| 1 year 6 months | 11.40 ± 1.12 | 80.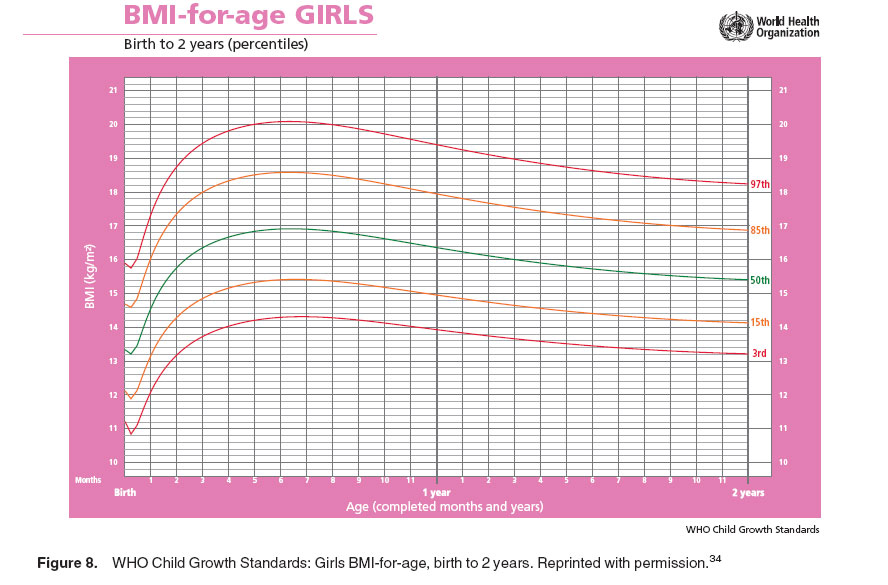 80 ± 2.98 80 ± 2.98 | 11.80 ± 1.18 | 81.73 ± 3.34 | |||
| 9000. 1 year | 12.27 ± 1.37 | 83.75 ± 3.57 | 12.67 ± 1.41 | 84.51 ± 2.85 | |||
| 12.6.63 ± 1.76 | 86.13 ± 3.87 | 13.04 ± 1.23 | 88.27 ± 3.70 | ||||
| 2 years 6 months | 13.93 ± 1.60 | 91.20 ± 4,28 | 13.96 ± 1.27 | 81.85 ± 3.78 | |||
| 3 years old | 14.85 ± 1.53 | 97.27 ± 3 , 78 | 14.95 ± 1.68 | 95.72 ± 3.68 | |||
| 4 years | 16.02 ± 2.30 | 100.56 ± 5.76 | 17, 14 ± 2.18 | 102.44 ± 4.74 | |||
| 5 years | 18.48 ± 2.44 | 109.00 ± 4.72 038 | 110.40 ± 5.14 | | ||||
| 6 years | 21.34 ± 3.14 | 115.70 ± 4.32 | 21. 20 20 | 115.98 ± 5.51 | |||
| 7 years old | 24.66 ± 4.08 | 123.60 ± 5.50 | 24.92 ± 4.44 | 123.88 ± 5.40 | |||
| 8 years | 27.48 ± 4.92 | 129.00 ± 5.48 | 27.86 ± 4.72 | 129.94 ± 5.70 | 0049 9 years old31.02 ± 5,92 | 136.96 ± 6.10 | 30.60 ± 5.86 | 9004.64 ± 6.12
| 10 years 10 years old | 888888888834.32 ± 6.40 | 140.30 ± 6.30 | 33.76 ± 5.26 | 140.33 ± 5.60 | |||
| years 11 years | 37.40 ± 7 06 | 144.58 ± 7.08 | 35.44 ± 6.64 | 143.38 ± 5.72 | |||
| 12 years 9004 038 | 152.81 ± 7.01 | 41.25 ± 7.40 | 150.05 ± 6.40 | ||||
| 48.70 ± 9.16 | 156.85 ± 6. 20 20 | 45.85 ± 8.26 | 156.65 ± 8.00 | ||||
| 14 years old | 51.32 ± 7.30 | 160.86 ± 6.36 | 51 , 18 ± 7.34 | 162.62 ± 7.34 | |||
| 15 years old | 56.65 ± 9.85 | 161.80 ± 7.40 | 56.50 ± 13.50 ± 13.50 | 168.10 ± 9.50 | |||
| 16 years old | 58.00 ± 9.60 | 162.70 ± 7.50 | 62.40 ± 14.10 | 172.60 ± 9.40 | |||
| 17 years old | 58.60 ± 9.40 | 163.10 ± 7.30 | 67.35 ± 12.75 | 176.30 | |||
Deviations of weight or height from tabular values
There is no need to panic if there is a minimal discrepancy with the indicated values in the table, and here's why:
- First of all, the child's height and weight charts contain reference indicators , what should ideally be the weight and height of the child, without taking into account many other factors .
 Sometimes parents of premature babies mistakenly use a standard table for comparison, while there are special tables for assessing the development of children born prematurely.
Sometimes parents of premature babies mistakenly use a standard table for comparison, while there are special tables for assessing the development of children born prematurely. - The rate of growth and weight gain for each child is unique . In the first year of life, babies develop in leaps and bounds. For example, during the period of introducing complementary foods, the weight of the baby may not reach the “norm” due to adaptation to a new type of food, and not because of pathology.
This does not mean that deviations from the norm should be ignored , but it is better to regard them as an occasion to pay attention and consult a specialist in order to identify possible health problems, or to make sure that they are not present.
What can cause obvious deviations from the norm?
Earlier we talked about minor deviations from the norm and that there is no need to be scared if your child is not growing and gaining weight strictly according to the chart.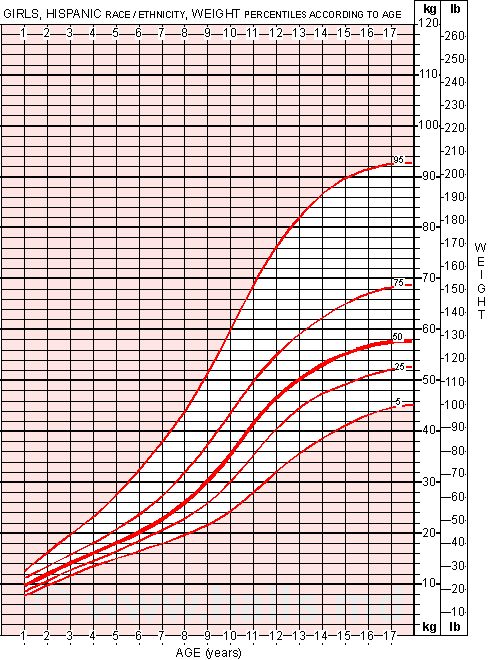 But what to do if the values of the essential have gone beyond the limits of the permissible parameters , or are they at the intersection of norm and pathology?
But what to do if the values of the essential have gone beyond the limits of the permissible parameters , or are they at the intersection of norm and pathology?
Reasons for possible deviations can be divided into two groups:
1. Non-endocrine:
- Constitutional growth retardation . Or in another way, the syndrome of late puberty. One of the variants of the norm, when the puberty jump occurs later than in other children.
- Family stunting . It has a hereditary predisposition, in the family of such children there are relatives with short stature. Growth retardation manifests itself from early childhood.
- Prematurity, intrauterine and postnatal injuries.
- Genetic syndromes . As a rule, they have many clinical manifestations, one of which is growth retardation.
- Chronic diseases of the cardiovascular, bronchopulmonary systems, gastrointestinal tract, as well as anemia.

- Fasting .
- Taking certain medications .
2. Endocrine:
- Growth hormone deficiency . Biologically active substance, which is the main regulator of the growth process after 2 years.
- Deficiency of thyroid hormones . More often of a congenital nature, it is clinically characterized by a delay in physical and intellectual development from birth.
- Type 1 diabetes mellitus . A disease in which, due to insulin deficiency, the flow of glucose into the cells of the body is impaired, the so-called. "starvation" of cells, as a result, growth rates slow down.
- Itsenko-Cushing's disease (or syndrome) . At the same time, the production of hormones of the adrenal cortex, glucocorticoids, is increased, which in large doses leads to a violation of the secretion of growth hormone.
- Rickets .
 A lack of vitamin D leads to bone destruction and skeletal deformities, which in turn is manifested, among other things, by a decrease in growth.
A lack of vitamin D leads to bone destruction and skeletal deformities, which in turn is manifested, among other things, by a decrease in growth. - Other rare disorders of the endocrine system.
As you can see, there are a lot of reasons.
If the child's growth is stunted, parents should consult a doctor to identify the causes of short stature and correct it in a timely manner.
Which specialist should I contact? First, you should make an appointment with a pediatrician. Also, in most cases, consultation with a pediatric endocrinologist is required.
Remember that for the normal growth of the child you need a complete, balanced diet with enough vitamins and minerals, as well as dosed physical activity.
Children's height and weight standards - WHO data
Children's height and weight standards - WHO data
A child's height and weight are parameters that parents are most concerned about. What are the norms of height and weight for children of different ages? We invite you to familiarize yourself with the data of the World Health Organization. Based on large-scale studies, scientists have established normal parameters for the development of children, which can be relied upon.
What are the norms of height and weight for children of different ages? We invite you to familiarize yourself with the data of the World Health Organization. Based on large-scale studies, scientists have established normal parameters for the development of children, which can be relied upon.
The height and weight of a child is the most exciting topic for parents
One of the most common questions that all mothers have is the rate of growth and weight of the child in the first months of the baby's life. Based on the recommended norms, you can understand whether your child is developing correctly and whether it is worth taking him to the doctor. A child's height and weight are important parameters by which parents can evaluate a child's health.
Often, parents are faced with rather conflicting information about what weight and height of a child is normal. Moreover, different doctors may interpret the current indicators in a child in different ways.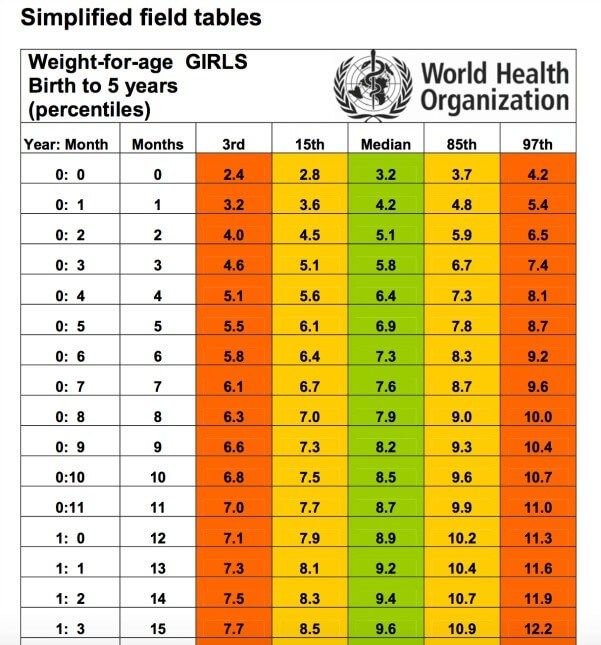 We hasten to inform you that the World Health Organization has established height and weight standards for boys and girls. This is the most up-to-date data on which to rely when interpreting the parameters of height and weight of children.
We hasten to inform you that the World Health Organization has established height and weight standards for boys and girls. This is the most up-to-date data on which to rely when interpreting the parameters of height and weight of children.
Standards of weight and height of a child, which are widely used today, in fact, do not reflect the real state of affairs - how exactly a child should grow and develop in order for his health to be in the best possible condition. Such data simply shows how the average child grows.
With regard to the standards developed by WHO, these data are more than just reference parameters for height and weight. The WHO tables on the norms of height and weight of children enable parents to determine the optimal values for the physical development of babies, taking into account the weight and height of children of different ages.
Child height and weight: how the norms were set
The 2002 UNICEF and WHO guidelines state that breastfeeding is the best form of feeding for babies.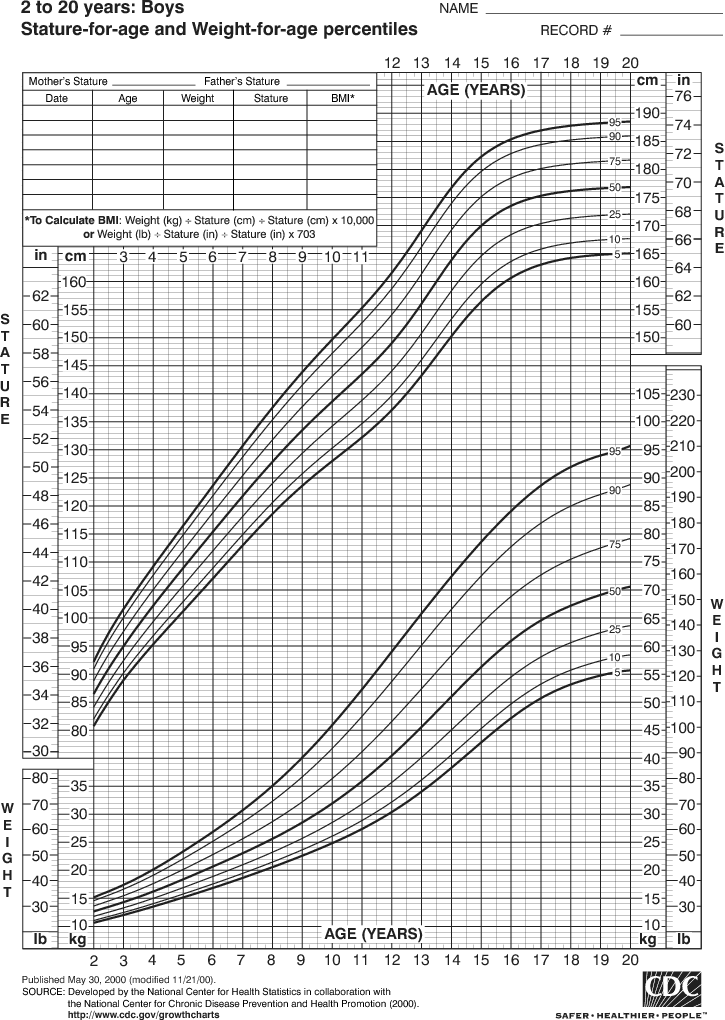 Mother's milk is the ideal food for the healthy growth and development of children. During the first six months, experts from WHO and UNICEF recommend feeding children exclusively with breast milk. After this period, children must receive adequate complementary foods for adequate growth and development. In this case, breastfeeding should continue up to two years or more (at the request of the mother).
Mother's milk is the ideal food for the healthy growth and development of children. During the first six months, experts from WHO and UNICEF recommend feeding children exclusively with breast milk. After this period, children must receive adequate complementary foods for adequate growth and development. In this case, breastfeeding should continue up to two years or more (at the request of the mother).
One of the distinguishing features of modern norms for the development and growth of children is the understanding of breastfeeding as a certain biological norm. A healthy child, not overweight and breastfeeding, was taken as a reference. In this regard, the new norms for the growth and weight of babies differ from those that were adopted on the basis of an analysis of the parameters of all children (who were both breastfed and bottle-fed).
To establish new norms for the development of children's growth, experts examined about 9thousands of children raised in a supportive environment that includes breastfeeding, a healthy diet, and the prevention of infectious diseases and other negative manifestations.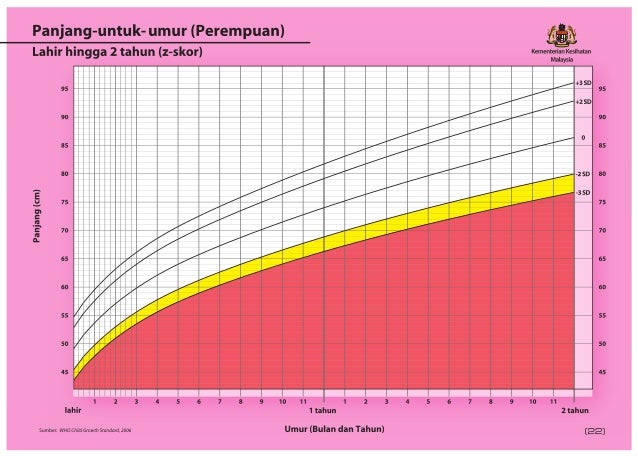 Moreover, the mothers of these children refrained from bad habits during pregnancy and breastfeeding. It was a large-scale project sponsored by the World Health Organization and a number of UN non-governmental organizations. As a result of the data obtained, graphs of weight and height were drawn up for boys and girls aged 0 to 10 years. It is noteworthy that these graphs show not only the absolute values of height and weight, but also the relationship with each other, and this ratio is very important for understanding how harmoniously a child develops. WHO tables will help calculate the norm of weight and height of a child.
Moreover, the mothers of these children refrained from bad habits during pregnancy and breastfeeding. It was a large-scale project sponsored by the World Health Organization and a number of UN non-governmental organizations. As a result of the data obtained, graphs of weight and height were drawn up for boys and girls aged 0 to 10 years. It is noteworthy that these graphs show not only the absolute values of height and weight, but also the relationship with each other, and this ratio is very important for understanding how harmoniously a child develops. WHO tables will help calculate the norm of weight and height of a child.
WHO Table No. 1: Height (in cm) and weight (in kg) of boys in the first year of life
By three months, boys grow to 61.4 cm and weigh 6.400 g. Low values will be parameters below 59.4 cm 5.700 g, and high values will be values above 63.5 cm and 7.200 g.
The age of 6 months is considered an important milestone in a child's development.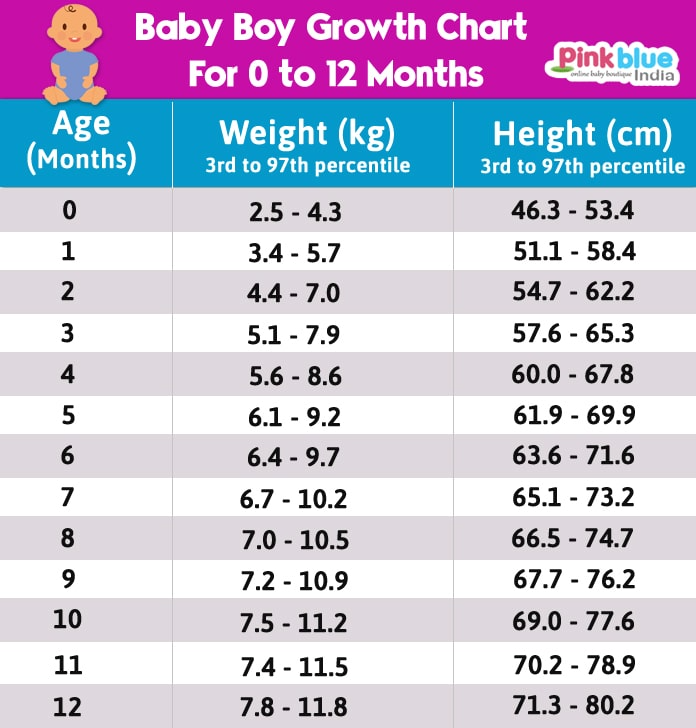 A six-month-old girl should grow to 65.7 cm and weigh 7,300 g.
A six-month-old girl should grow to 65.7 cm and weigh 7,300 g.
WHO Table 3: Height (in cm) of a boy under 10
WHO Table 4: Weight (in kg) of a boy under 10
At 10, boys are normal should reach the parameters of 137.8 cm 31.200 g. Figures less than 131.4 cm and 26.700 g are assessed as low, and figures above 144.2 cm and 37.000 g are considered high.
WHO Chart 5: Girl's height (in cm) under 10
WHO Chart 6: Girl's weight (in kg) under 10
A 10-year-old girl should have an average height of 138.55 cm and a mass of 31.900 g. Data less than 132.2 cm 27.100 g are considered low, and values above 145 cm 38.200 g are considered high.
How to determine the correct height and weight of a child
At home, you can use a home height meter or a measuring tape to change the height of a child. Place the child barefoot on the floor with their back to the ruler.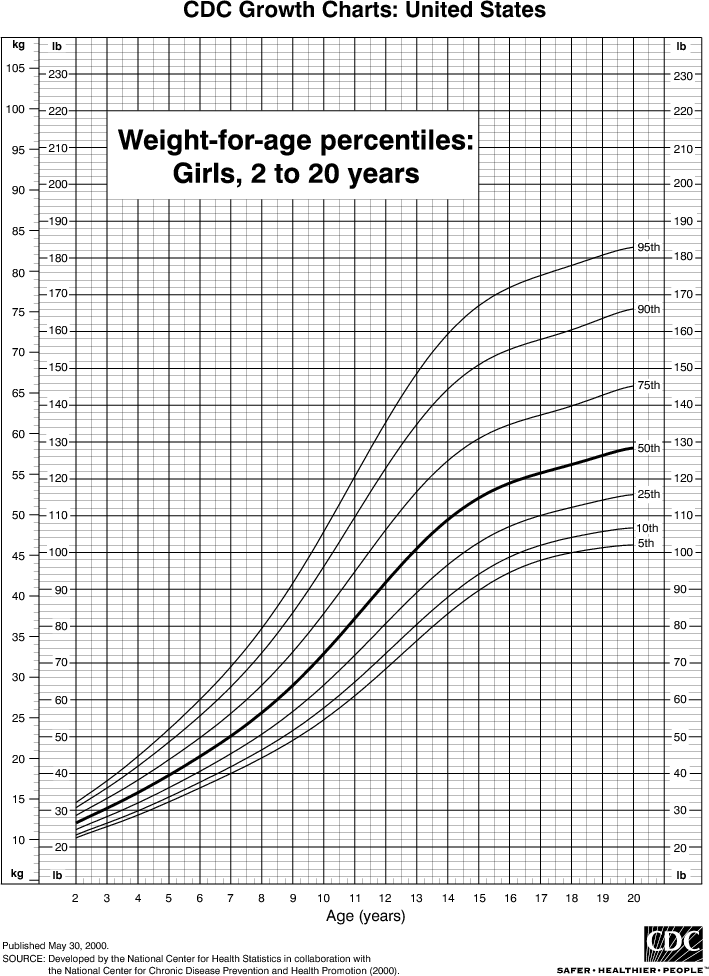 Make sure that the baby's body is straight, and the arms are lowered along the body, the feet are tightly shifted, and the knees are extended. The child's head should be positioned in such a way that the edge of the lower eyelid and the upper edge of the hearing aid are on the same horizontal plane. During the measurement of height, the child should touch the wall with the shoulder blades, buttocks and heels. Find out in our ranking of the top 10 online casinos which gaming clubs withdraw winnings to a bank account. Attach a flat object perpendicular to the stadiometer and mark the height readings on the scale.
Make sure that the baby's body is straight, and the arms are lowered along the body, the feet are tightly shifted, and the knees are extended. The child's head should be positioned in such a way that the edge of the lower eyelid and the upper edge of the hearing aid are on the same horizontal plane. During the measurement of height, the child should touch the wall with the shoulder blades, buttocks and heels. Find out in our ranking of the top 10 online casinos which gaming clubs withdraw winnings to a bank account. Attach a flat object perpendicular to the stadiometer and mark the height readings on the scale.
As for the child's body weight, it is determined on the scales. Most often these are electronic scales. Make sure that the child is in the center of the scales. Depending on the age of the child, you need to weigh him in a lying, sitting or standing position. If you weigh a small child in a diaper, then the weight of the diaper should be subtracted from the total mass. Weigh the child in the morning, before feeding, when the child urinates and empties.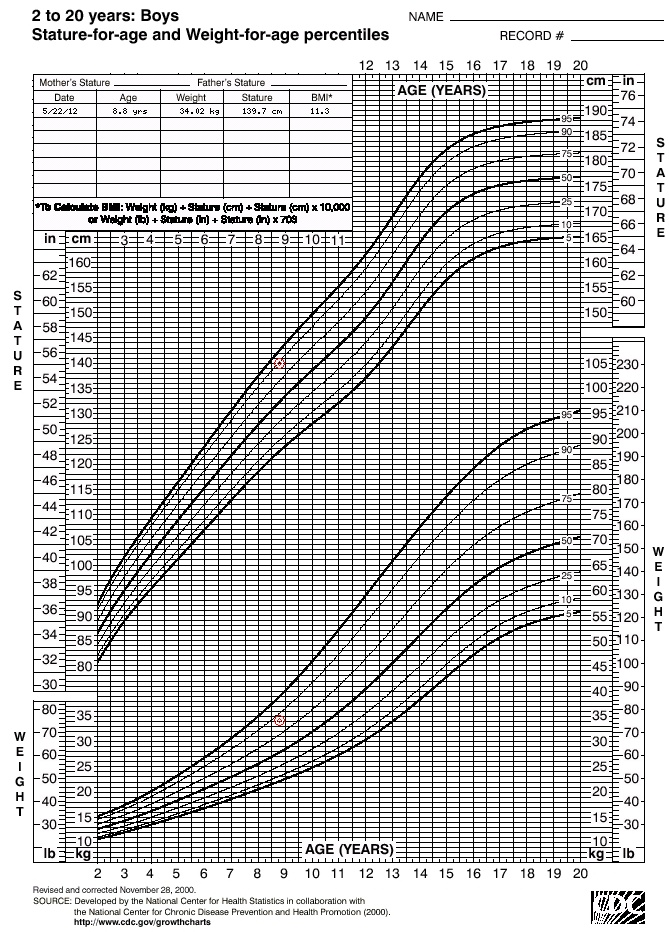
Child's weight: causes of abnormalities
In some cases, the child may have problems with weight. Too much or too little weight can indicate certain problems or specific conditions. In particular, deviations from the norm are possible for the following reasons:
Energy imbalance. The most common reason is getting more calories than you need. This leads to weight gain. And when a child receives fewer calories than he needs to maintain normal life, this, on the contrary, leads to weight loss. Children who eat food that is equivalent in energy balance to their lifestyle do not have weight problems. Thus, the main causes of abnormal body weight are: increased food intake, malnutrition or low physical activity.
Diseases. In some cases, weight problems are possible due to the development of certain diseases and disorders, for example, when the hormonal background changes, when the metabolism is disturbed.
The most common problem for parents is overfeeding a child when he does not want to eat, but he is forced to.