Pelvic cavity diagram
Anatomy, Abdomen and Pelvis, Female Pelvic Cavity - StatPearls
Introduction
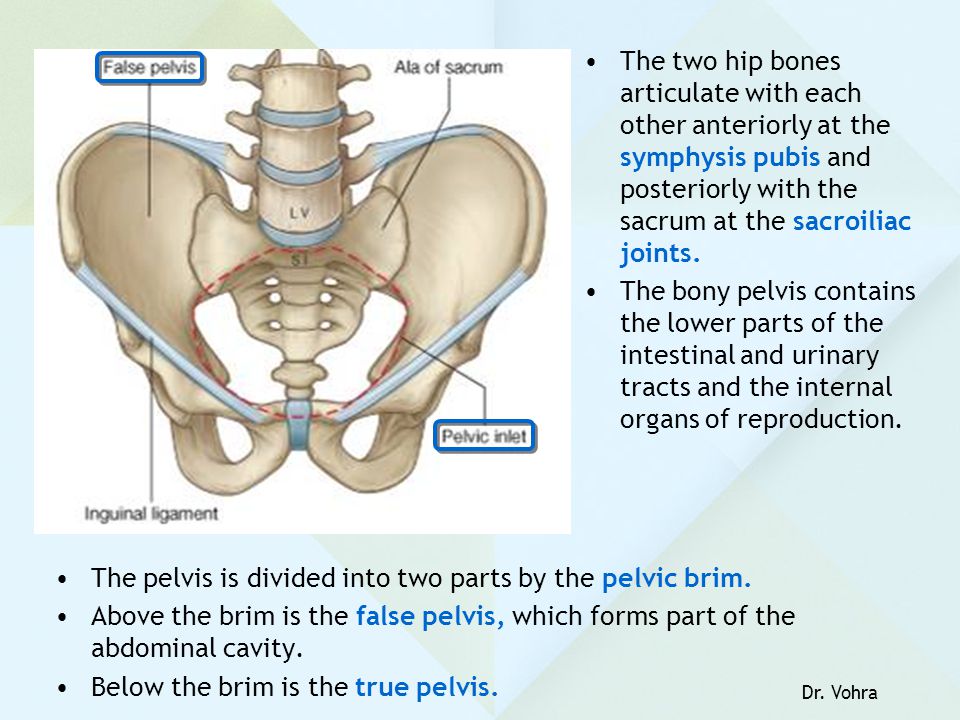
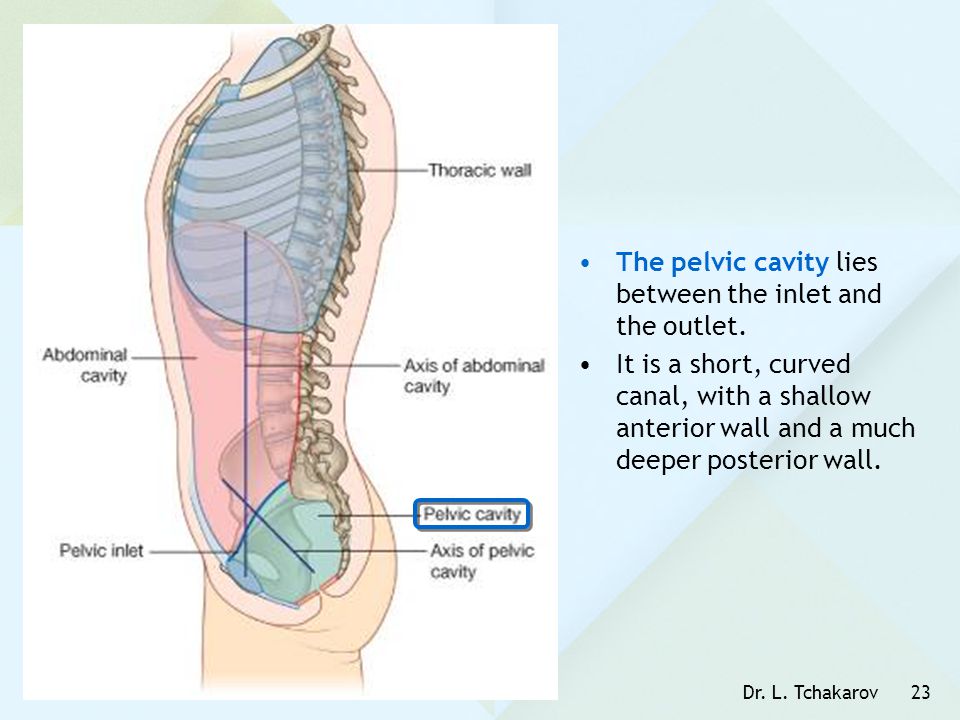
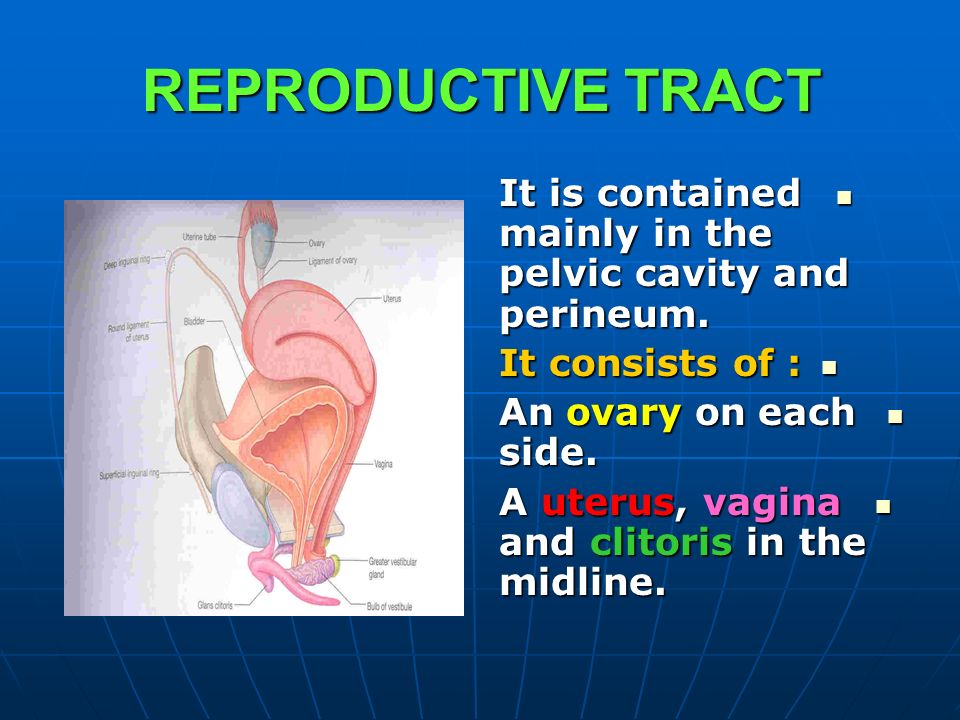
The pelvic cavity is a bowl-like structure that sits below the abdominal cavity. The true pelvis, or lesser pelvis, lies below the pelvic brim (Figure 1). This landmark begins at the level of the sacral promontory posteriorly and the pubic symphysis anteriorly. The space below contains the bladder, rectum, and part of the descending colon. In females, the pelvis also houses the uterus, fallopian tubes, and ovaries. Knowledge of anatomy unique to females is essential for all clinicians, especially those in the field of obstetrics and gynecology.
Structure and Function
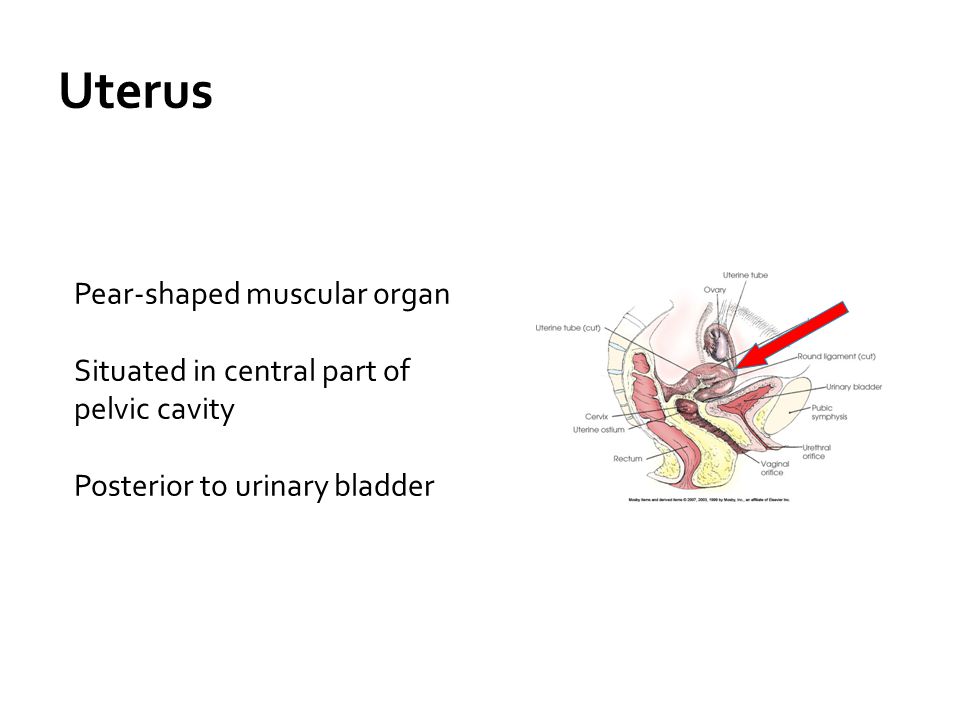
The uterus sits in the center of the female pelvic cavity (Figure 2.) The most common position of the uterus in the pelvic cavity is anteverted and anteflexed.[1] "Version" refers to the angle between the cervix and the vagina. An anteverted uterus appears "tipped forward" in the pelvic cavity. A retroverted uterus is "tipped backward. " Retroversion is a normal variant but can lead to dyspareunia. Additionally, retroversion of a gravid uterus correlates with higher rates of vaginal bleeding and spontaneous abortion.[2]
"Flexion" is the term for the angle between the cervix and uterine body. Anteflexed means the uterus is bent forward. Retroflexed means the uterus bends backward. Occasionally, retroflexion is seen after cesarean section and may be due to scar tissue that attaches the uterine body to the abdominal wall, causing the fundus to bend posteriorly.[3] However, the data supporting this theory is limited.
Anterior to the uterus is the bladder, with rectum located posteriorly. Between the uterus and the rectum is the recto-uterine space, also known as the posterior cul-de-sac. It is a potential space prone to fluid collection. Small amounts of physiologic fluid accumulate during ovulation and menses. Pathologic causes of fluid collection in the recto-uterine pouch include pelvic abscesses, drop metastasis from gastrointestinal malignancies, and endometriosis.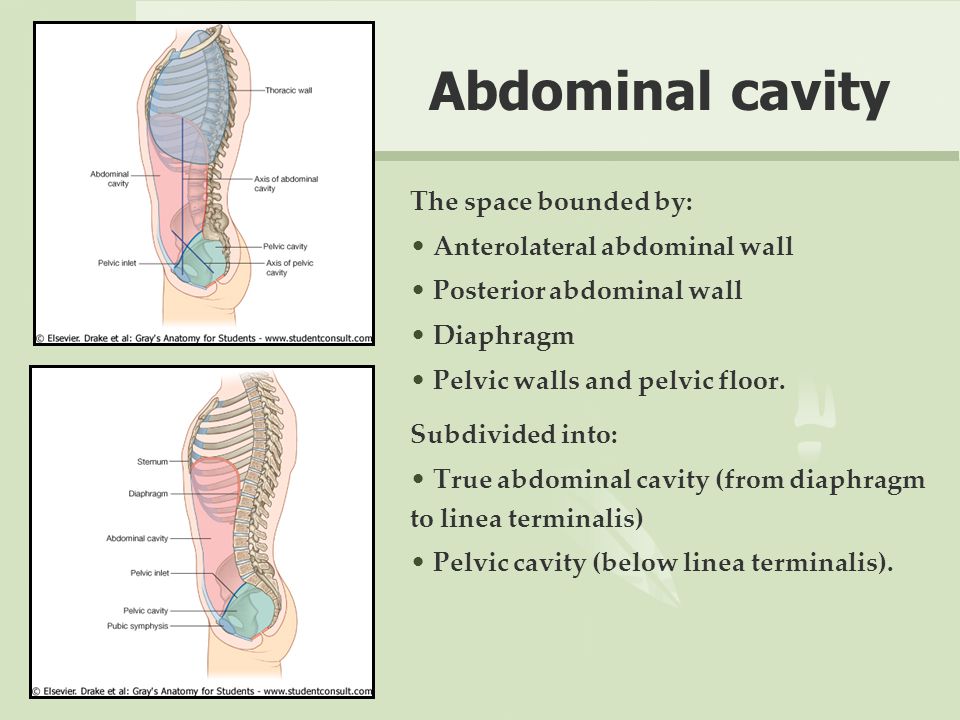 In certain situations, if fluid accumulation is severe, this space can be drained by performing a culdocentesis, which is accomplished by inserting a needle through the posterior fornix of the upper vagina to access the posterior cul-de-sac.
In certain situations, if fluid accumulation is severe, this space can be drained by performing a culdocentesis, which is accomplished by inserting a needle through the posterior fornix of the upper vagina to access the posterior cul-de-sac.
The posterior cul-de-sac communicates with the retroperitoneal space of the abdomen via the right and left epiploic gutters. The right gutter leads to the hepatorenal space, also known as Morrison's pouch. The right epiploic gutter also allows the spread of pelvic pathogens into the subphrenic space. Occasionally infection of the subphrenic space can occur, leading to adhesions on the capsule of the liver. This pathology is known as Fitz-Curtis-Hugh syndrome or gonococcal perihepatitis.
The left epiploic gutter leads to the splenorenal pouch. Due to the leftward position of the rectum, pelvic pathology is less likely to spread to the abdomen via the left epiploic communication.[4]
Embryology
The organs of the female reproductive tract each have a unique embryological origin. The exact embryological timeline in which these organs develop is still open to debate because most embryologic studies use animal models with different gestational ages. However, there is a consensus that the ovaries are the first to develop. They arise from the surface of the mesonephros at the gonadal ridge.[5] Later in development, the ovaries descend into the pelvis with guidance from the gubernaculum. The inferior aspect of the gubernaculum subsequently becomes the round ligament of the uterus and terminates at the labia majora.
The exact embryological timeline in which these organs develop is still open to debate because most embryologic studies use animal models with different gestational ages. However, there is a consensus that the ovaries are the first to develop. They arise from the surface of the mesonephros at the gonadal ridge.[5] Later in development, the ovaries descend into the pelvis with guidance from the gubernaculum. The inferior aspect of the gubernaculum subsequently becomes the round ligament of the uterus and terminates at the labia majora.
In females, the absence of a Y chromosome allows the uterus to form. It derives from the Müllerian ducts, also known as the paramesonephric ducts. These ducts fuse to form the uterus, fallopian tubes, and cervix. Some studies suggest that the paramesonephric ducts also give rise to the upper vagina while other studies indicate that the vagina exclusively derives from the urogenital sinus epithelium.[6] In males, a substance coded for on the Y chromosome, known as the anti-Mullerian hormone, prevents the formation of internal female reproductive organs.
Blood Supply and Lymphatics
Arterial
The anterior branch of the internal iliac artery supplies most of the female reproductive organs. The uterine artery supplies the majority of the uterus (Figure 3). The lower uterine segment has a dual blood supply that includes branches of the vaginal artery. The ovaries are an exception because they receive blood from the ovarian arteries, which descend from the abdominal aorta.
The superior vesicle artery supplies the upper bladder. In females, the vaginal artery supplies the lower bladder. Both arteries are also branches of the anterior branch of the internal iliac artery.
The rectum receives vascular supply via three vessels. The superior rectal artery is the terminal branch of the inferior mesenteric artery. The middle rectal is a branch of the internal iliac artery. The inferior rectal is a branch of the pudendal artery.
Venous
The venous supply of pelvic organs follows the arterial supply.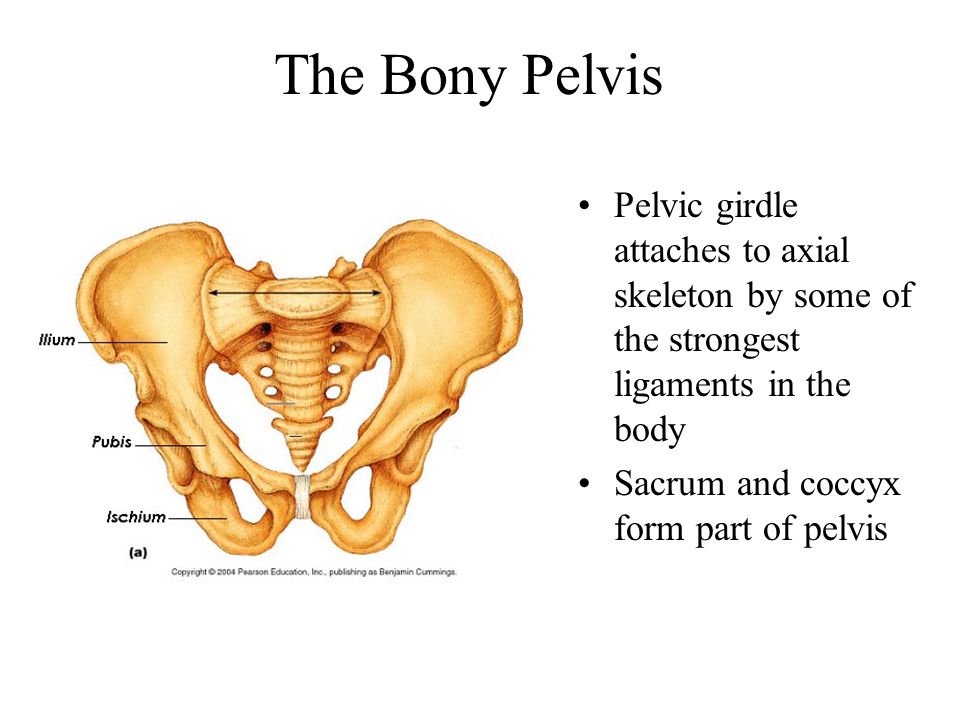 The uterine vein receives blood from the uterus and drains into the internal iliac vein. The ovarian veins receive blood from the ovaries. The right ovarian vein drains its contents directly into the inferior vena cava, while the left ovarian vein drainage is into the left renal vein. The increased length of the left ovarian vein makes it more susceptible to compression, especially during pregnancy.[7] Ovarian vein compression can lead to pelvic venous compression syndrome. The resulting pelvic vasculature congestion is a cause of chronic pelvic pain and may occur in non-pregnant patients as well.
The uterine vein receives blood from the uterus and drains into the internal iliac vein. The ovarian veins receive blood from the ovaries. The right ovarian vein drains its contents directly into the inferior vena cava, while the left ovarian vein drainage is into the left renal vein. The increased length of the left ovarian vein makes it more susceptible to compression, especially during pregnancy.[7] Ovarian vein compression can lead to pelvic venous compression syndrome. The resulting pelvic vasculature congestion is a cause of chronic pelvic pain and may occur in non-pregnant patients as well.
The left-sided venous supply is also unique because the left internal iliac artery travels from its right-sided origin at the inferior vena cava towards a leftward destination in the pelvis. The longer path makes the left internal iliac more prone to compression and may explain why venous thromboembolism in pregnancy most commonly occur in the left iliac and iliofemoral veins.[8] Additionally, the leftward position of the sigmoid colon causes a gravid uterus to tip toward the right, which is thought to increase the risk of iliac vessel compression further.
Lymphatics
The lymphatic network of the pelvis is complex but is essential to understand when staging and treating gynecologic malignancies. Generally, the pelvic organs drain into the internal and external iliac lymph nodes (Figure 5).
The lymphatic drainage of the uterus is more complicated and remains somewhat ambiguous.[9] Some researchers suggest it may involve pelvic and para-aortic lymph nodes.[10] A more recent study from 2017 suggests that the uterus has two primary routes of lymphatic drainage, an upper pathway that drains to the external iliac and/or obturator lymph nodes and a lower pathway that drains to the internal iliac and/or presacral lymph nodes.[11]
The ovaries are an exception to the other female pelvic organs because they do not drain to pelvic lymph nodes. Their lymphatic drainage follows their blood supply; therefore they drain directly to the paraaortic lymph nodes.
Nerves
The female reproductive organs have both autonomic and sensory innervation.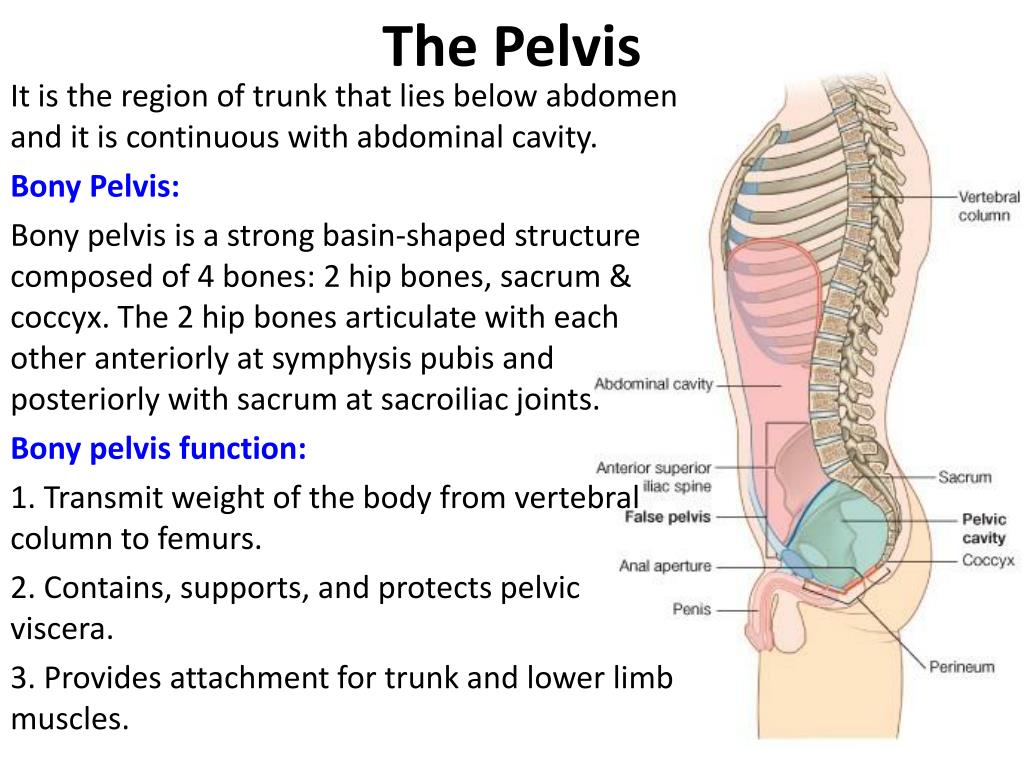 Beginning with the autonomic nervous system, sympathetic fibers exit at the level of T10 to L2 to form the superior hypogastric plexus, which divides into the left and right hypogastric nerve at approximately the level of the sacral promontory. The parasympathetic nerve fibers exit at the level of S2 to 4 and meet up with the sympathetic nervous system at the right and left hypogastric nerves. The right and left hypogastric nerves then migrate inferiorly to form the inferior hypogastric plexus. After this point, the nerve fibers follow blood vessels to their target organs. The inferior hypogastric plexus also receives sensory information from the uterus.
Beginning with the autonomic nervous system, sympathetic fibers exit at the level of T10 to L2 to form the superior hypogastric plexus, which divides into the left and right hypogastric nerve at approximately the level of the sacral promontory. The parasympathetic nerve fibers exit at the level of S2 to 4 and meet up with the sympathetic nervous system at the right and left hypogastric nerves. The right and left hypogastric nerves then migrate inferiorly to form the inferior hypogastric plexus. After this point, the nerve fibers follow blood vessels to their target organs. The inferior hypogastric plexus also receives sensory information from the uterus.
The ovarian nerve innervates the ovary. Although previously thought only to contain sensory fibers, recent animal studies suggest this nerve also carries autonomic fibers that may play a role in hormone secretion and constriction of ovarian vessels.[12][13][14] Recent studies suggest that the cervix and upper vagina also have autonomic innervation; however, the role of autonomic innervation in this region remains unclear. [15][16] Sensory innervation to the cervix and upper vagina has been more widely studied and receives supply by the pelvic splanchnic nerves. The pudendal nerve supplies the sensory innervation of the lower vagina. Pudendal nerve blocks can be used to provide local pain relief to laboring women by using the ischial spines as landmarks. Although once the treatment of choice for labor pain, it is no longer commonly used due to the widespread use of epidural anesthesia.[17]
[15][16] Sensory innervation to the cervix and upper vagina has been more widely studied and receives supply by the pelvic splanchnic nerves. The pudendal nerve supplies the sensory innervation of the lower vagina. Pudendal nerve blocks can be used to provide local pain relief to laboring women by using the ischial spines as landmarks. Although once the treatment of choice for labor pain, it is no longer commonly used due to the widespread use of epidural anesthesia.[17]
Muscles
The inferior border of the pelvic cavity is the pelvic diaphragm. It is made up of a group of muscles. From posterior to anterior, these muscles include:
Piriformis
Coccygeus
Iliococcygeus
Pubococcygeus
Puborectalis
The fibers of the iliococcygeus, pubococcygeus, and puborectalis make up the levator ani muscle. Because of its proximity to the vagina, the pubococcygeus and puborectalis are the most commonly injured muscles during vaginal deliveries.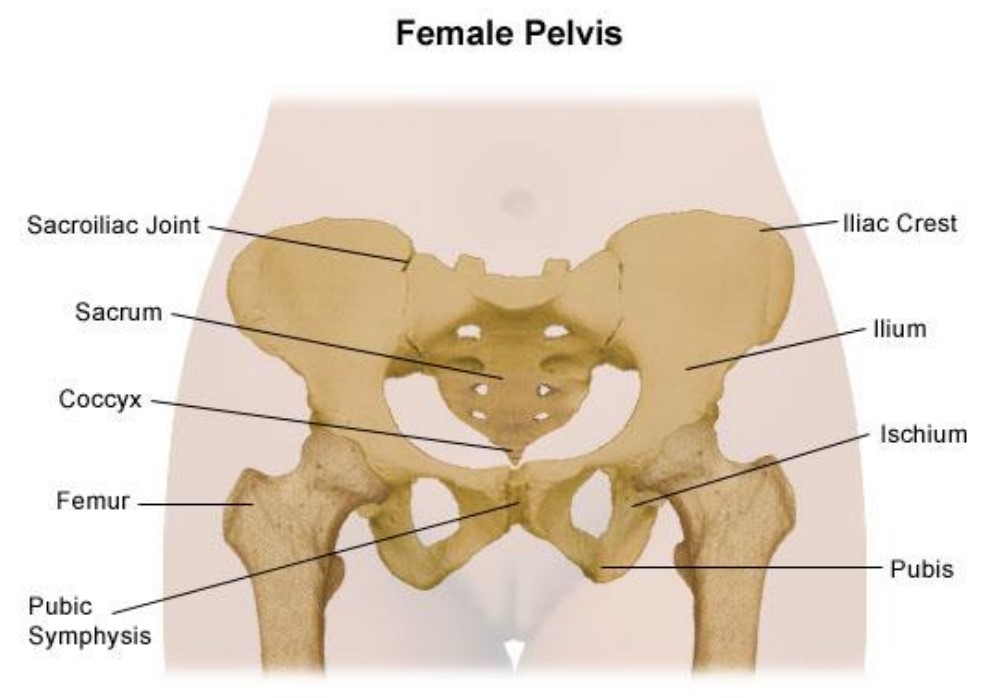 [18] The obturator internus muscles make up the peripheral borders of the pelvis but are not among the muscles of the pelvic floor.
[18] The obturator internus muscles make up the peripheral borders of the pelvis but are not among the muscles of the pelvic floor.
Ligaments
Three ligaments anchor the uterus. The uterosacral ligament supports the uterus posteriorly, and the pubocervical ligament anchors the uterus anteriorly. The transverse cervical ligament supports the uterus laterally. Unlike the anterior and posterior planes that contain the bladder and rectum respectively, the lateral plane lacks supporting structures other than the transverse cervical ligament. It is for this reason that this ligament also has the name of the "cardinal" ligament. The transverse ligament also differs from other supporting ligaments of the uterus because it is the only ligament that contains a vasculature structure, the uterine artery.
The ovary also has ligamentous support. The utero-ovarian ligament, also known as the ovarian ligament, extends from the ovary to the uterine body. The ovary is supported superiorly by the infundibulopelvic ligament, also known as the suspensory ligament of the ovary.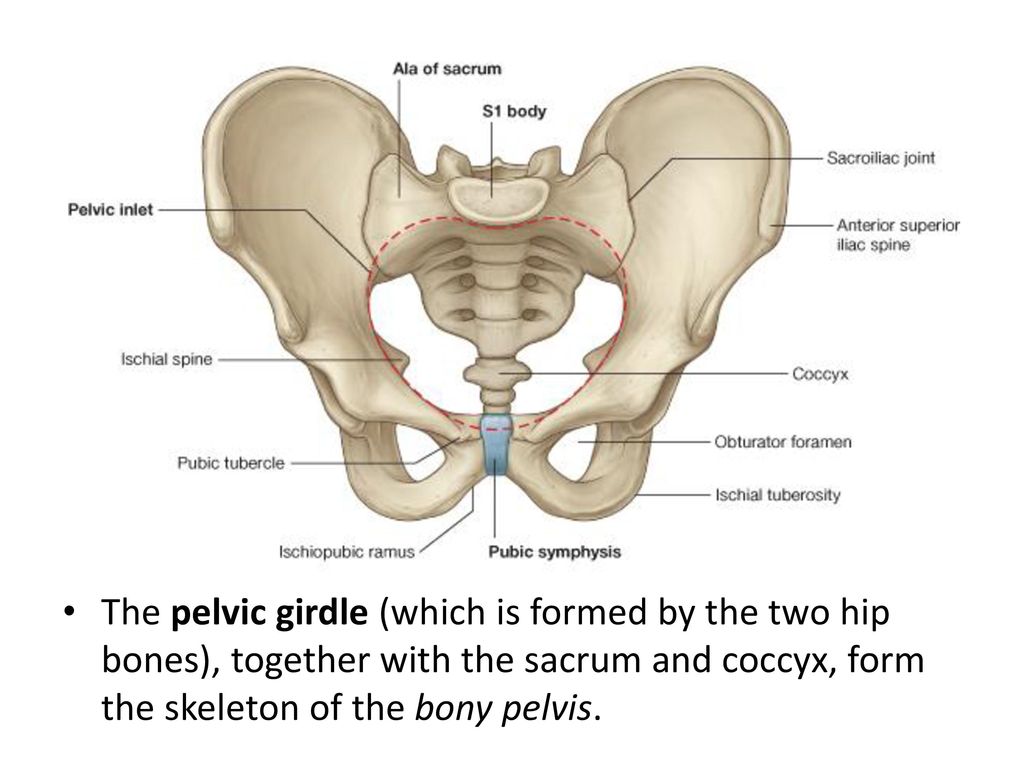 This ligament descends from the lateral aspect of the abdominal wall and contains the ovarian neurovascular bundle.
This ligament descends from the lateral aspect of the abdominal wall and contains the ovarian neurovascular bundle.
The broad ligament overlies the uterus, fallopian tubes, and ovaries. It is the inferior most extension of the parietal peritoneum and has three divisions based on location. The lateral most aspect of the broad ligament is the "mesovarium" and overlies the ovaries. The "mesosalpinx" covers the fallopian tubes. The largest portion of the broad ligament is the "mesometrium" and overlies the uterus.
Physiologic Variants
The uterine and ovarian arteries supply the majority of the female reproductive tract. The uterine artery, like many pelvic arteries, has a variable presentation. It most commonly arises from the anterior branch of the internal iliac artery and shares a common trunk with the obliterated umbilical artery.[19] One study that analyzed imaging from 218 patients reported this presentation in 80.7 % of cases.[20] The same study reported the uterine artery branched directly off of the internal iliac in 13.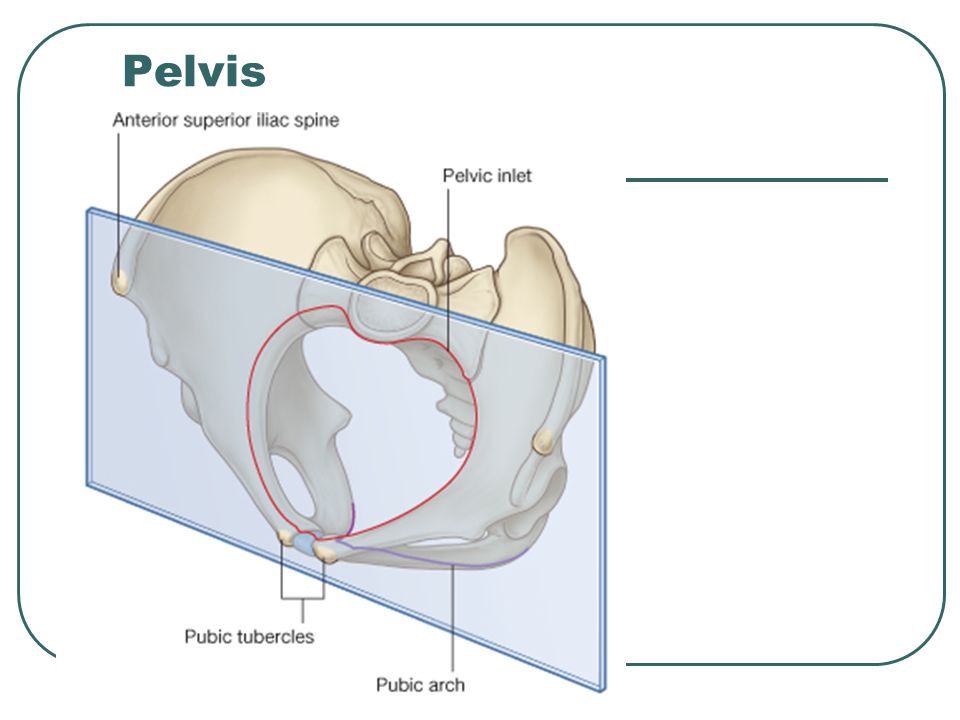 6% of cases, making this the most common variation. The second and third most common variations they found were direct branching from the superior gluteal artery and internal pudendal artery, respectively. These variations are necessary to be aware of during surgery as well as during uterine artery embolization.
6% of cases, making this the most common variation. The second and third most common variations they found were direct branching from the superior gluteal artery and internal pudendal artery, respectively. These variations are necessary to be aware of during surgery as well as during uterine artery embolization.
Ovarian artery variants are less common, but case reports exist that detail unique aberrations. One case report found an aberrant ovarian artery arising from the external iliac artery.[21] Another study reported an ovarian artery that branched directly from the common iliac artery.[22] These variations are thought to be due to abnormal descent of the ovaries into the pelvis during embryological development and may also correlate to other differences.[23]
Surgical Considerations
Several anatomical relationships are essential for surgeons to be aware of when operating in the female pelvis. For example, during a cesarean section, the bladder should always be identified to avoid iatrogenic cystotomy.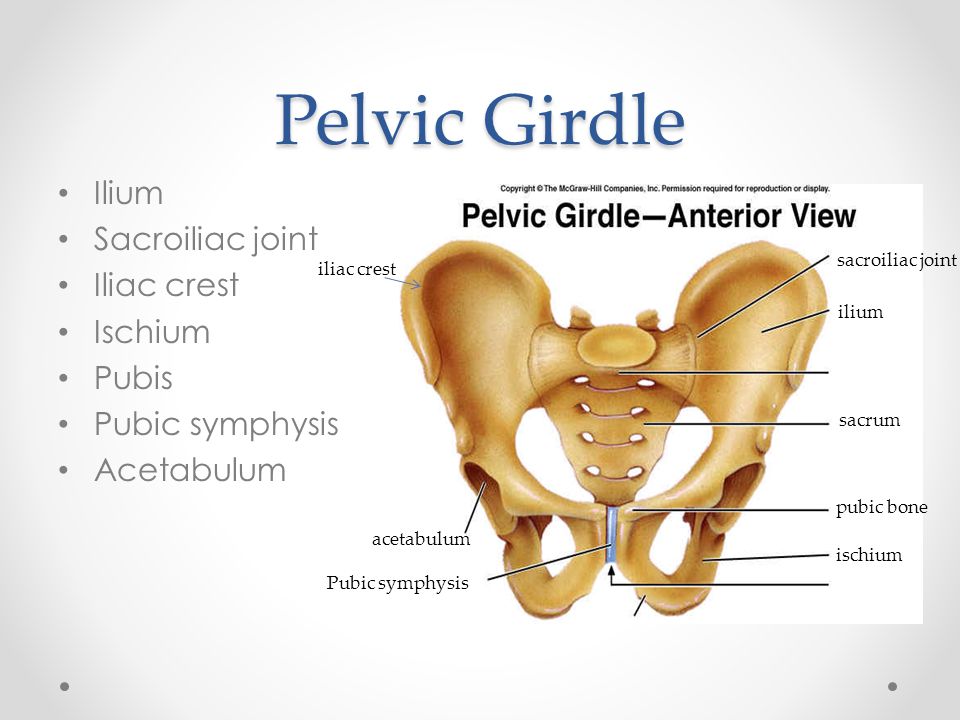 This cautionary measure is especially the case in patients that have had a prior cesarean section because scar tissue can cause the bladder to adhere to the anterior uterine wall.
This cautionary measure is especially the case in patients that have had a prior cesarean section because scar tissue can cause the bladder to adhere to the anterior uterine wall.
During any uterine surgery, identification of the uterine artery is vital. If cut, massive bleeding can ensue. During abdominal hysterectomies, the uterine artery is typically “skeletonized” so that its path along the uterus is clearly identifiable to the operating team.
If hemorrhage does occur, knowledge of pelvic vasculature becomes crucial. If the bleeding vessel cannot be clearly identified, the internal iliac should be clamped below the origin of the superior gluteal artery. This method is preferred so that necrosis of the gluteal muscle does not occur.
When operating deeper in the female pelvis, identification of the ureter is also crucial. There are three major locations where this structure may exist. Beginning superiorly, the ureters descend into the pelvis posterior to the infundibulopelvic ligaments. The ureters maintain this relationship until approximately the level of the iliac vessels, where they begin to travel more medially.
The ureters maintain this relationship until approximately the level of the iliac vessels, where they begin to travel more medially.
As the ureters continue to travel inferiorly, the next important landmark is the transverse cervical ligament. The ureters dive under this structure. Awareness of this relationship is of considerable importance when performing a hysterectomy. A popular pneumonic used by medical students is, "water under the bridge."
After passing under the transverse cervical ligament, the ureters continue to travel medially toward the bladder. Their insertion into the inferior aspect of the bladder is the third major location they should undergo positive identification intraoperatively. The insertion points are also visible from inside the bladder itself, during cystoscopy; this is sometimes performed after pelvic surgery if an injury to the bladder is suspected.
Injury to the bladder can also occur during pelvic surgery from the vaginal approach. When operating in this plane, injury to the rectum is also a possibility because at this level the rectum is directly posterior to the vagina (Figure 6. ) Avoiding bladder and rectal injury becomes increasingly difficult if the patient has pelvic organ prolapse, such as cystocele or rectocele.
) Avoiding bladder and rectal injury becomes increasingly difficult if the patient has pelvic organ prolapse, such as cystocele or rectocele.
When performing surgery on the fallopian tubes, such as during a tubal ligation or tubal anastomosis, the location of the round ligament should be determined. Due to the similarity in structure and location, the round ligament can be mistaken for a fallopian tube. Unlike the round ligaments, however, the fallopian tubes have fimbriae, a characteristic can be used to differentiate between these two structures intraoperatively.
Clinical Significance
Clinical correlates related to female pelvic anatomy can be summarized as follows:
The standard position of the uterus is anteverted and anteflexed. Abnormal positioning of the uterus is associated with pathology. Retroversion, for example, is a cause of dyspareunia. Additionally, retroversion of a gravid uterus is associated with higher rates of spontaneous abortion.
The posterior cul-de-sac, located between the uterus and the rectum, is a potential space prone to fluid collection.
 Physiologic fluid accumulates during menses and ovulation. If fluid collection is pathologic, this space can undergo drainage via culdocentesis.
Physiologic fluid accumulates during menses and ovulation. If fluid collection is pathologic, this space can undergo drainage via culdocentesis.The posterior cul-de-sac communicates with the abdomen via the left and right epiploic gutters, which allows the spread of pelvic pathogens into the abdominal cavity. Due to the leftward position of the rectum, infections usual take the path of the right epiploic gutter. The right epiploic gutter leads to potential spaces surrounding the liver. These include the hepatorenal space, also known as Morrison’s pouch, and the subphrenic space. Infection of the subphrenic space secondary to a gonococcal pelvic infection is termed Fitz-Curtis-Hugh syndrome or gonococcal perihepatitis.
The increased length of the left ovarian vein makes it more susceptible to compression, especially during pregnancy. Compression of this vessel sometimes leads to pelvic venous compression syndrome and is a cause of chronic pelvic pain in both pregnant and non-pregnant patients.
Venous thromboembolism in pregnancy is most commonly left-sided and occur in the iliofemoral vessels, which is thought to be because of pelvic vessel engorgement in combination with the increased path the left iliac vein takes across the pelvis. These factors make this vessel more susceptible to compression by a gravid uterus.
Understanding the lymphatic drainage of the female reproductive tract is important when tracking the spread of gynecologic malignancies. Generally, the female reproductive organs drain to the internal and external iliac lymph nodes. A notable exception is the ovaries, which drain to the paraaortic lymph nodes.
The pudendal nerve receives sensory innervation to the lower vagina. Historically, pudendal nerve blocks were used to alleviate labor pains. However, pudendal nerve blocks are no longer commonly practiced due to the wide-spread use of epidural anesthesia.
The muscles of the pelvic floor are susceptible to injury during vaginal deliveries.
 The most commonly injured muscles are the pubococcygeus and puborectalis muscles due to their proximity to the vagina.
The most commonly injured muscles are the pubococcygeus and puborectalis muscles due to their proximity to the vagina.The pelvic vasculature contains many physiologic variants that are important for surgeons to know. Interventional radiologists should also be knowledgeable of variants, particularly during uterine artery embolization to treat fibroids. The uterine artery most commonly arises from the anterior branch of the internal iliac and shares a trunk with the obliterated umbilical artery. The most common variation is direct branching from the internal iliac.
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
Figure
Compilation of 6 images detailing anatomy of female pelvic cavity. Contributed by Gray's Anatomy Plates (Public Domain)
References
- 1.
Roach MK, Andreotti RF. The Normal Female Pelvis. Clin Obstet Gynecol. 2017 Mar;60(1):3-10.
 [PubMed: 28005593]
[PubMed: 28005593]- 2.
Weekes AR, Atlay RD, Brown VA, Jordan EC, Murray SM. The retroverted gravid uterus and its effect on the outcome of pregnancy. Br Med J. 1976 Mar 13;1(6010):622-4. [PMC free article: PMC1639005] [PubMed: 1252851]
- 3.
Sanders RC, Parsons AK. Anteverted retroflexed uterus: a common consequence of cesarean delivery. AJR Am J Roentgenol. 2014 Jul;203(1):W117-24. [PubMed: 24951223]
- 4.
Turco G, Chiesa GM, de Manzoni G. [Echographic anatomy of the greater peritoneal cavity and its recesses]. Radiol Med. 1988 Jan-Feb;75(1-2):46-55. [PubMed: 3279472]
- 5.
Yao HH. The pathway to femaleness: current knowledge on embryonic development of the ovary. Mol Cell Endocrinol. 2005 Jan 31;230(1-2):87-93. [PMC free article: PMC4073593] [PubMed: 15664455]
- 6.
Robboy SJ, Kurita T, Baskin L, Cunha GR. New insights into human female reproductive tract development. Differentiation.
 2017 Sep - Oct;97:9-22. [PMC free article: PMC5712241] [PubMed: 28918284]
2017 Sep - Oct;97:9-22. [PMC free article: PMC5712241] [PubMed: 28918284]- 7.
Jeanneret C, Beier K, von Weymarn A, Traber J. Pelvic congestion syndrome and left renal compression syndrome - clinical features and therapeutic approaches. Vasa. 2016;45(4):275-82. [PubMed: 27428495]
- 8.
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy. Obstet Gynecol. 2018 Jul;132(1):e1-e17. [PubMed: 29939938]
- 9.
Coleman RL, Frumovitz M, Levenback CF. Current perspectives on lymphatic mapping in carcinomas of the uterine corpus and cervix. J Natl Compr Canc Netw. 2006 May;4(5):471-8. [PubMed: 16687095]
- 10.
Burke TW, Levenback C, Tornos C, Morris M, Wharton JT, Gershenson DM. Intraabdominal lymphatic mapping to direct selective pelvic and paraaortic lymphadenectomy in women with high-risk endometrial cancer: results of a pilot study.
 Gynecol Oncol. 1996 Aug;62(2):169-73. [PubMed: 8751545]
Gynecol Oncol. 1996 Aug;62(2):169-73. [PubMed: 8751545]- 11.
Geppert B, Lönnerfors C, Bollino M, Arechvo A, Persson J. A study on uterine lymphatic anatomy for standardization of pelvic sentinel lymph node detection in endometrial cancer. Gynecol Oncol. 2017 May;145(2):256-261. [PubMed: 28196672]
- 12.
Uchida S, Kagitani F. Autonomic nervous regulation of ovarian function by noxious somatic afferent stimulation. J Physiol Sci. 2015 Jan;65(1):1-9. [PMC free article: PMC4276811] [PubMed: 24966153]
- 13.
Pastelín CF, Rosas NH, Morales-Ledesma L, Linares R, Domínguez R, Morán C. Anatomical organization and neural pathways of the ovarian plexus nerve in rats. J Ovarian Res. 2017 Mar 14;10(1):18. [PMC free article: PMC5351206] [PubMed: 28292315]
- 14.
Cruz G, Fernandois D, Paredes AH. Ovarian function and reproductive senescence in the rat: role of ovarian sympathetic innervation. Reproduction. 2017 Feb;153(2):R59-R68.
 [PubMed: 27799628]
[PubMed: 27799628]- 15.
Mónica Brauer M, Smith PG. Estrogen and female reproductive tract innervation: cellular and molecular mechanisms of autonomic neuroplasticity. Auton Neurosci. 2015 Jan;187:1-17. [PMC free article: PMC4412365] [PubMed: 25530517]
- 16.
Mowa CN. Uterine Cervical Neurotransmission and Cervical Remodeling. Curr Protein Pept Sci. 2017;18(2):120-124. [PubMed: 27001061]
- 17.
Schrock SD, Harraway-Smith C. Labor analgesia. Am Fam Physician. 2012 Mar 01;85(5):447-54. [PubMed: 22534222]
- 18.
Memon HU, Handa VL. Vaginal childbirth and pelvic floor disorders. Womens Health (Lond). 2013 May;9(3):265-77; quiz 276-7. [PMC free article: PMC3877300] [PubMed: 23638782]
- 19.
Peters A, Stuparich MA, Mansuria SM, Lee TT. Anatomic vascular considerations in uterine artery ligation at its origin during laparoscopic hysterectomies. Am J Obstet Gynecol. 2016 Sep;215(3):393.e1-3. [PubMed: 27287682]
- 20.
Chantalat E, Merigot O, Chaynes P, Lauwers F, Delchier MC, Rimailho J. Radiological anatomical study of the origin of the uterine artery. Surg Radiol Anat. 2014 Dec;36(10):1093-9. [PubMed: 24052200]
- 21.
Kwon JH, Kim MD, Lee KH, Lee M, Lee MS, Won JY, Park SI, Lee DY. Aberrant ovarian collateral originating from external iliac artery during uterine artery embolization. Cardiovasc Intervent Radiol. 2013 Feb;36(1):269-71. [PubMed: 22565531]
- 22.
Kim WK, Yang SB, Goo DE, Kim YJ, Chang YW, Lee JM. Aberrant ovarian artery arising from the common iliac artery: case report. Korean J Radiol. 2013 Jan-Feb;14(1):91-3. [PMC free article: PMC3542308] [PubMed: 23323036]
- 23.
Rahman HA, Dong K, Yamadori T. Unique course of the ovarian artery associated with other variations. J Anat. 1993 Apr;182 ( Pt 2):287-90. [PMC free article: PMC1259840] [PubMed: 8376204]
Pelvic cavity: Anatomical spaces | Kenhub
Author: Lorenzo Crumbie MBBS, BSc • Reviewer: Dimitrios Mytilinaios MD, PhD
Last reviewed: July 27, 2022
Reading time: 11 minutes
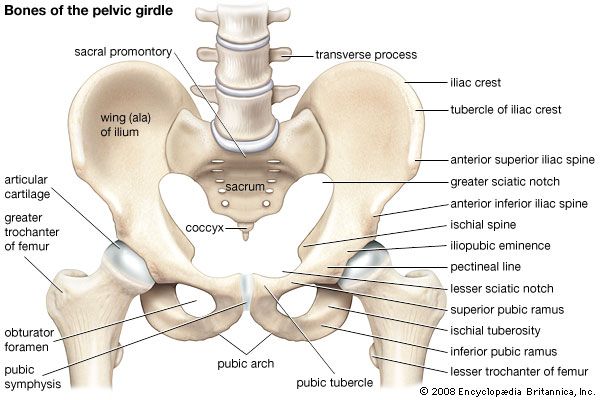
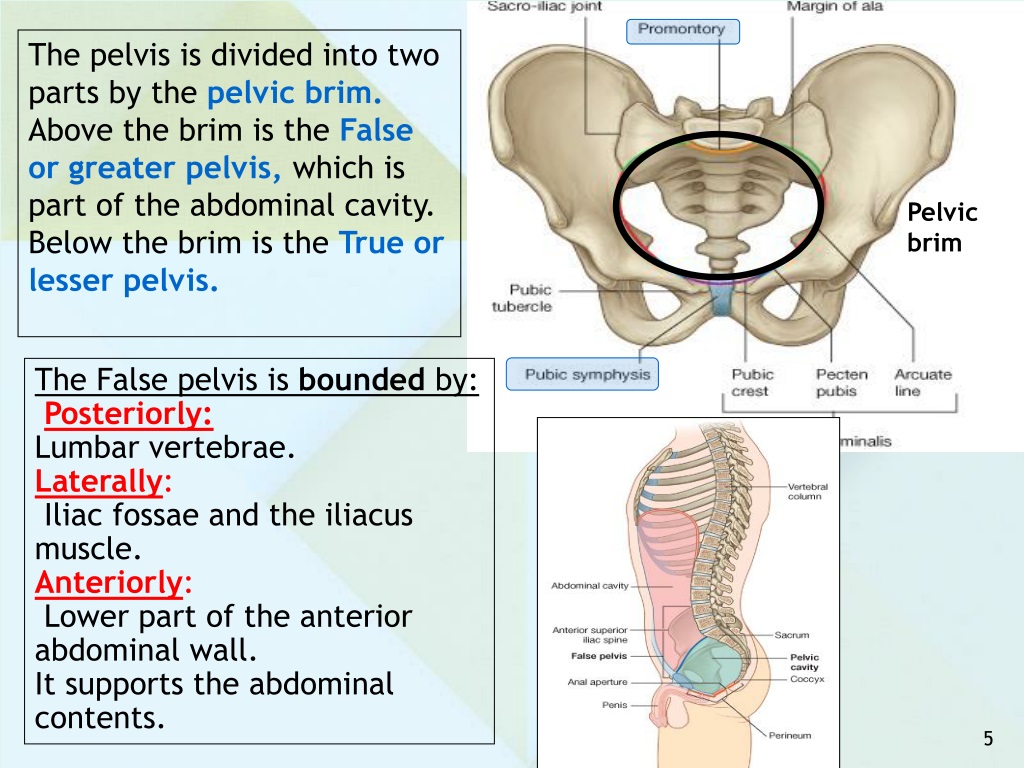
The pelvic cavity is formed by three bilateral pairs of bones (pubis, ilium and ischium) and two posteriorly located bones (sacrum and coccyx).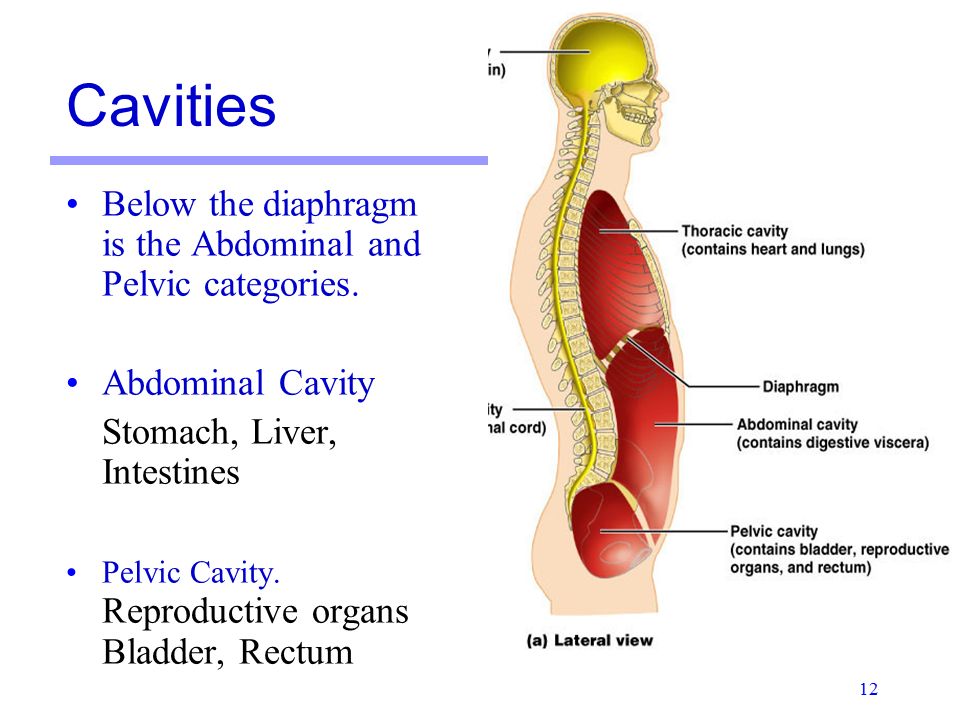 The cavity is home to the some of the urinary organs, most of the reproductive organs and the distal part of the digestive tract in humans. The pelvic cavity is described as having two parts:
The cavity is home to the some of the urinary organs, most of the reproductive organs and the distal part of the digestive tract in humans. The pelvic cavity is described as having two parts:
- There is a false pelvis that spans the region below the iliac crest and above the arcuate line (pectinate line, anteriorly)
- And there is a true pelvis that begins below the arcuate line.
The caudal end of the peritoneal cavity rests in the pelvic cavity. As a result, spaces associated with this region are also considered as being part of the pelvic cavity spaces. Additionally, there are other anatomical spaces that exist inferior to the peritoneum.
Since there are differences between the male and female internal and external reproductive organs, there are also some differences in the spaces of the pelvic cavity in that regards. This article aims to highlight the spaces and point out any gender-related differences.
Contents
- Rectovesical pouch (male)
- Rectouterine pouch of Douglas (female)
- Pararectal fossa
- Vesicouterine pouch (female)
- Rectovesical space (male)
- Ischiorectal (ischioanal) fossa
- Other pelvic spaces
- Summary
- Sources
+ Show all
Pelvic cavity (anterior view)Learn all the cavities of the body in half the time using our interactive quizzes and videos.
Cavities of the body Explore study unit
Rectovesical pouch (male)
The superior and upper posterior parts of the urinary bladder as well as the upper and middle part of the rectum are covered by a single layer of peritoneum. The peritoneal covering creates a continuous surface coursing over the superior part of the urinary bladder to the middle and upper rectum. A depression exists at the junction of the two surfaces that is referred to as the rectovesical pouch.
Rectovesical pouch (sagittal view)Rectouterine pouch of Douglas (female)
A similar situation to that previously described also exists in the female pelvis. However, the space has an additional structure. In the female pelvic cavity, the uterus and vagina occupy the space between the urinary bladder and the rectum. The peritoneum is continuous over all three structures and consequently, an additional space is created. The space between the middle and superior rectum and the uterus is known as the rectouterine pouch of Douglas.
The space between the middle and superior rectum and the uterus is known as the rectouterine pouch of Douglas.
Pararectal fossa
In both males and females, the rectovesical pouch and the rectouterine pouch of Douglas (respectively) not only communicate superiorly with the peritoneal cavity, but also bilaterally with the pararectal fossae. As suggested by the nomenclature, the spaces surround the intraperitoneal portion of the rectum. They are limited laterally (on either side) by the vesicosacral (uterosacral) folds in females and the sacrogenital folds in males. The pararectal fossa, rectovesical pouch and rectouterine pouch of Douglas are commonly occupied by loops of small intestines.
Have you been making any of these common anatomy learning mistakes?
Vesicouterine pouch (female)
The second pelvic space formed by peritoneal covering in females is the vesicouterine pouch. The space exists between the posterior surface of the urinary bladder and the anterior surface of the uterus. This space is also continuous superiorly with the peritoneal cavity. The broad ligament and the round ligament of the uterus are lateral and posterior to the space. Due to the fact that the uterus is most commonly found in an anteverted (bent forward) position, its anterior surface is more closely related to the posterosuperior surface of the urinary bladder than its posterior surface is to the intraperitoneal rectum.
Vesicouterine pouch (lateral-right view)Rectovesical space (male)
Inferior to the rectovesical pouch, is a region known as the rectovesical space.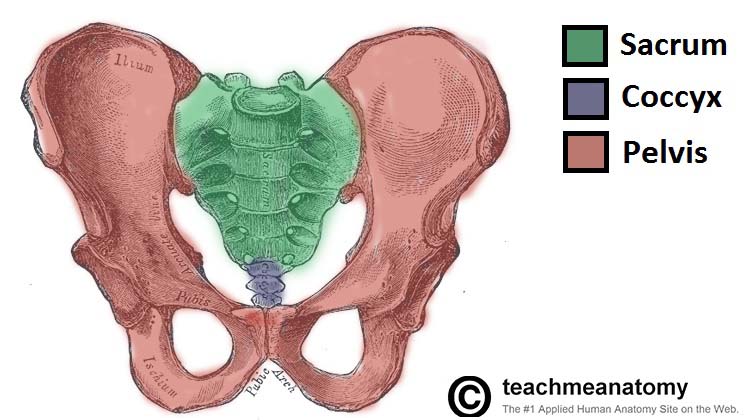 The space is so named as it is located posterior to the urinary bladder and prostate, and anterior to the distal third of the rectum (extraperitoneal part). The space is further divided into three compartments by a septum, known as the rectovesical or rectoprostatic fascia of Denonvillier, which extends from the apex of the rectovesical pouch to the deep and superficial transverse perineal muscles. The three spaces are:
The space is so named as it is located posterior to the urinary bladder and prostate, and anterior to the distal third of the rectum (extraperitoneal part). The space is further divided into three compartments by a septum, known as the rectovesical or rectoprostatic fascia of Denonvillier, which extends from the apex of the rectovesical pouch to the deep and superficial transverse perineal muscles. The three spaces are:
- The retrovesical part, which is the most superior of the three subdivisions. It is anterior to Denonvillier’s fascia and posterior to the urinary bladder. It also contains the seminal vesicles.
- The retroprostatic part is the most inferior part of the space. The posteroinferior part of the prostate gland and the posterior fibers of the sphincter urethrae are anterior to the space and Denonvillier’s fascia is posterior to it.
- Finally, the prerectal part of the space spans the full length of Denonvillier’s fascia.
 However, it is situated posterior to the septum and anterior to the distal third of the rectum; with the anterior rectal fascia being its closest posterior relation. The deep fibers of the external anal sphincter muscles and its fascia are immediately related to the inferior part of the space.
However, it is situated posterior to the septum and anterior to the distal third of the rectum; with the anterior rectal fascia being its closest posterior relation. The deep fibers of the external anal sphincter muscles and its fascia are immediately related to the inferior part of the space.
In females, the homologue to Denonvillier’s fascia is the rectovaginal fascia. A congenital abnormality, known as rectovaginal fistula would traverse the rectovaginal space, pierce the fascia and permit faecal transmission into the vagina. This defect can be corrected surgically.
Want to learn more about anatomy basics? Learn with quizzes in our 101 guide to basic medical terminology.
Ischiorectal (ischioanal) fossa
Bilateral to the inferior aspect of the rectum and the anus are a pair of triangular spaces known as the ischioanal fossae.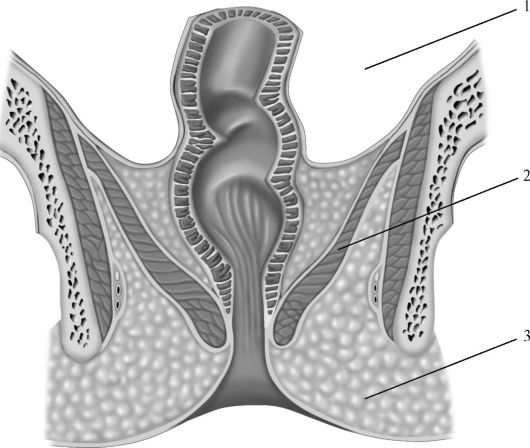 The apex of the space is located laterally, where its roof and lateral walls meet. The former is formed by the obliquely coursing levator ani muscle along with the inferior fascia of the pelvic diaphragm. The latter is formed by two structures: superiorly by the obturator internus muscle and its fascia and inferiorly by the medial part of the ischial tuberosity.
The apex of the space is located laterally, where its roof and lateral walls meet. The former is formed by the obliquely coursing levator ani muscle along with the inferior fascia of the pelvic diaphragm. The latter is formed by two structures: superiorly by the obturator internus muscle and its fascia and inferiorly by the medial part of the ischial tuberosity.
Medially, the ischioanal fossa is limited by the medial part of levator ani (superiorly) and the external anal sphincter muscles (inferiorly). Finally, the perineal skin forms the floor of the region. The anterobasal and posterobasal constraints of the fossa are the posterior aspect of the perineal body along with the muscles of the urogenital diaphragm, and the gluteus maximus and the posterior sacrotuberous ligament, respectively.
The ischioanal fossa houses several neurovascular and connective tissue structures.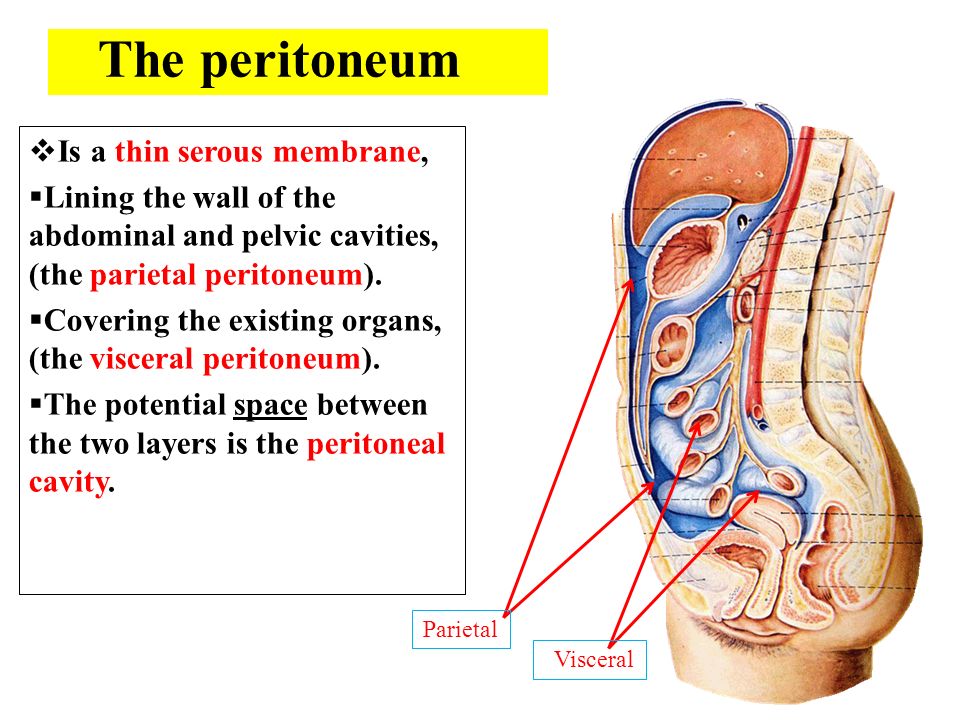 There are adipose lobules that gradually become smaller superoinferiorly. In the inferolateral wall, a neurovascular bundle courses through a tunnel formed in the fascia of obturator internus known as Alcock’s (pudendal) canal. Through this conduit, the internal pudendal vessels and the pudendal and perineal nerves course to their points of supply.
There are adipose lobules that gradually become smaller superoinferiorly. In the inferolateral wall, a neurovascular bundle courses through a tunnel formed in the fascia of obturator internus known as Alcock’s (pudendal) canal. Through this conduit, the internal pudendal vessels and the pudendal and perineal nerves course to their points of supply.
Each pudendal neurovascular bundle enters the canal at the lesser sciatic notch and journey to the deep perineal pouch. The pudendal neurovascular bundle also gives off inferior rectal branches that cross the ischioanal fossa. Additionally, the posterior labial (scrotal) neurovascular structures (branches of the pudendal neurovascular bundle) transverse the front of the fossa while the perineal branch of the sacral plexus (S4) and the perforating cutaneous nerve cross the back of the fossa to access their target sites.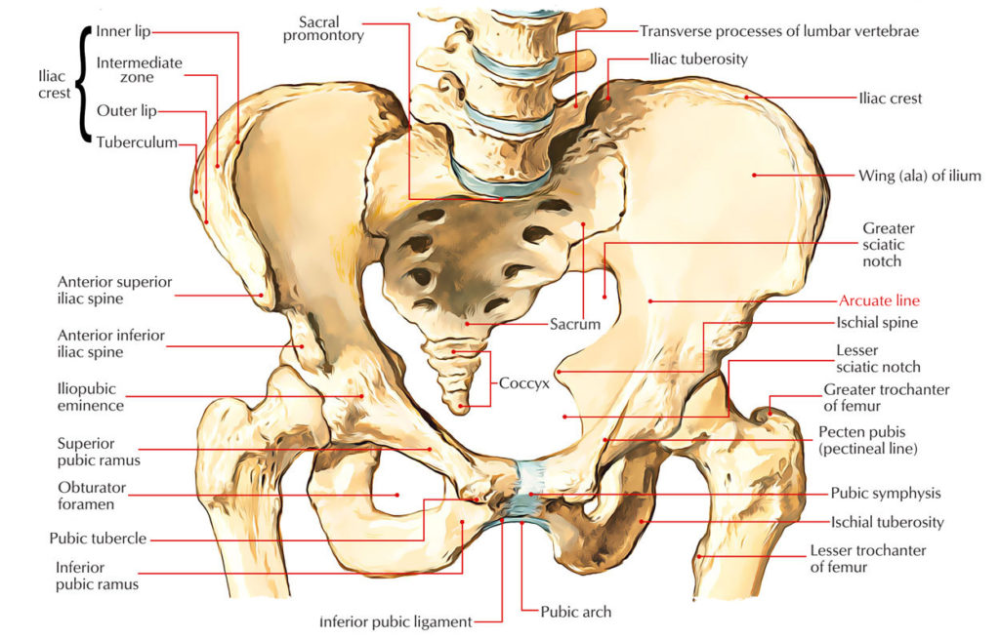
Infected abscesses located near the midline of one fossa cannot contaminate the opposite fossa because communication between the two regions is limited at this point. On the other hand, cross contamination of the fossae is possible via the retrosphincteric space.
To learn more about the anatomy of the ischiorectal fossa, check out this video:
Other pelvic spaces
In addition to the larger spaces (potential spaces) mentioned above, there are smaller spaces found within the pelvic cavity. These include:
- The retropubic (prevesical) space of Retzius, which is located between the symphysis pubis and the anterior border of the bladder (and prostate gland in males),
- Between the rectal fascia and sacral fascia, and superior to the levator ani muscle and superior fascia of the pelvic diaphragm, is the presacral space.

- There are two postanal spaces: a deep postanal space lies inferior to the levator ani muscle, superior to the anococcygeal ligament and anterior to the tip of the coccyx; the superficial postanal space lies superior to the skin of the buttocks, inferior to the anococcygeal ligament and posterior to the anal canal. The superficial postanal space also overlaps with part of the perianal space,
- Inferior and posterior to the bulbospongiosus muscle is the superficial perineal pouch. It is limited posteriorly (and simultaneously separated from the perianal space) by Colle’s fascia. Anteriorly, the superficial perineal compartment limited by Gallaudet’s fascia.
That's it - you're done! There's only one thing left to do: quiz your new-found knowledge.
Summary
The pelvic cavity is formed by three bilateral pairs of bones (pubis, ilium and ischium) and two posteriorly located bones (sacrum and coccyx).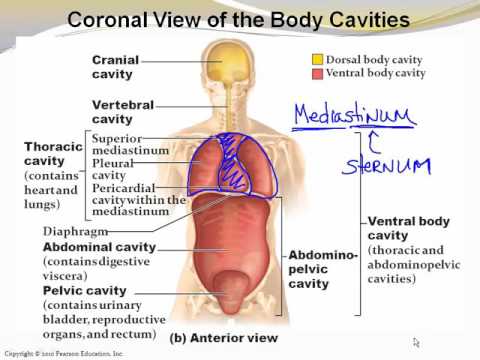 The cavity is home to the some of the urinary organs, most of the reproductive organs and the distal part of the digestive tract in humans. The spaces of the pelvic cavity are the following:
The cavity is home to the some of the urinary organs, most of the reproductive organs and the distal part of the digestive tract in humans. The spaces of the pelvic cavity are the following:
- Rectovesical Pouch (males)
- Rectouterine Pouch of Douglas (females)
- Pararectal Fossa
- Vesicouterine Pouch (females)
- Rectovesical Space (males)
- Ischioanal Fossa
- Retropubic Space of Retzius
- Presacral Space
- Postanal Space
- Perianal Space
- Superficial Perineal Pouch
Sources
All content published on Kenhub is reviewed by medical and anatomy experts. The information we provide is grounded on academic literature and peer-reviewed research. Kenhub does not provide medical advice.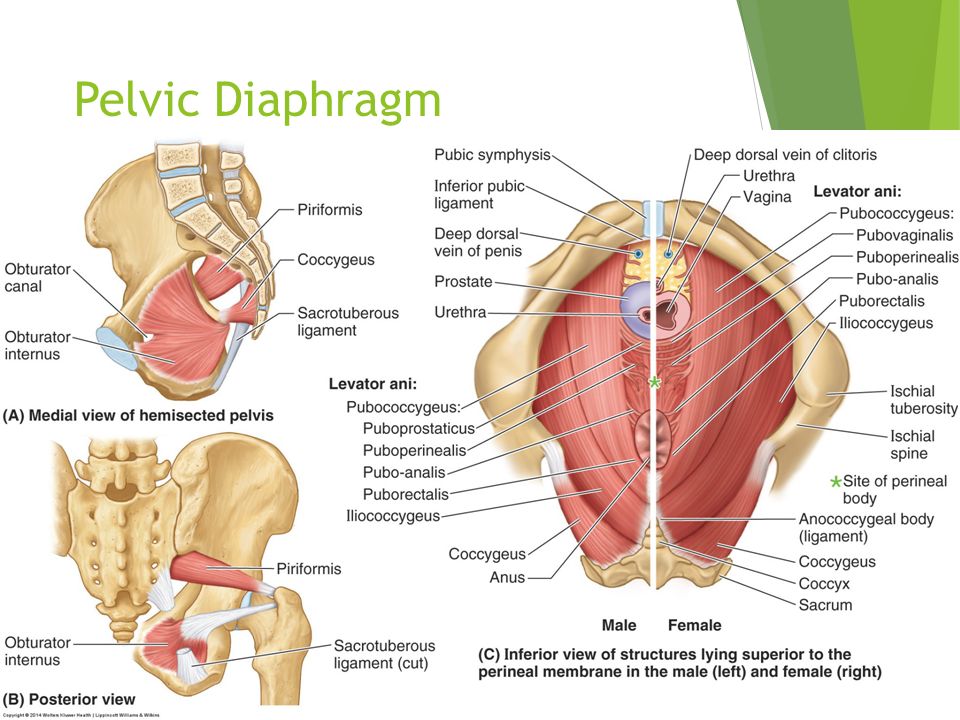 You can learn more about our content creation and review standards by reading our content quality guidelines.
You can learn more about our content creation and review standards by reading our content quality guidelines.
References:
- Ludwikowski, B., Hayward, I. and Fritsch, H. (2002). Rectovaginal fascia: An important structure in pelvic visceral surgery? About its development, structure, and function. Journal of Pediatric Surgery, 37(4), pp.634-638.
- Netter, F. (2014). Atlas of Human Anatomy. 6th ed. Philadelphia, PA: Saunders; Elservier, pp.321, 341, 350, 370, 374.
- Sinnatamby, C. and Last, R. (2011). Last's Anatomy. 12th ed. Edinburgh: Churchill Livingstone/Elsevier, pp.316-317.
- Zhai, L., Liu, J., Li, Y., Yuan, W. and He, L. (2009). Denonvilliers’ Fascia in Women and Its Relationship with the Fascia Propria of the Rectum Examined by Successive Slices of Celloidin-Embedded Pelvic Viscera.
 Diseases of the Colon & Rectum, 52(9), pp.1564-1571.
Diseases of the Colon & Rectum, 52(9), pp.1564-1571.
Illustrators:
- Pelvic cavity (anterior view) - Paul Kim
- Rectovesical pouch (sagittal view) - Irina Münstermann
- Rectouterine pouch (lateral-right view) - Irina Münstermann
- Vesicouterine pouch (lateral-right view) - Irina Münstermann
- Ischioanal fossa (anterior view) - Samantha Zimmerman
- Pudendal neurovascular bundle (ventral view) - Samantha Zimmerman
- Inferior rectal artery (posterior view) - Begoña Rodriguez
- Retropubic space (sagittal view) - Paul Kim
- Presacral space (superior view) - Paul Kim
Anatomical spaces of the pelvic cavity: want to learn more about it?
Our engaging videos, interactive quizzes, in-depth articles and HD atlas are here to get you top results faster.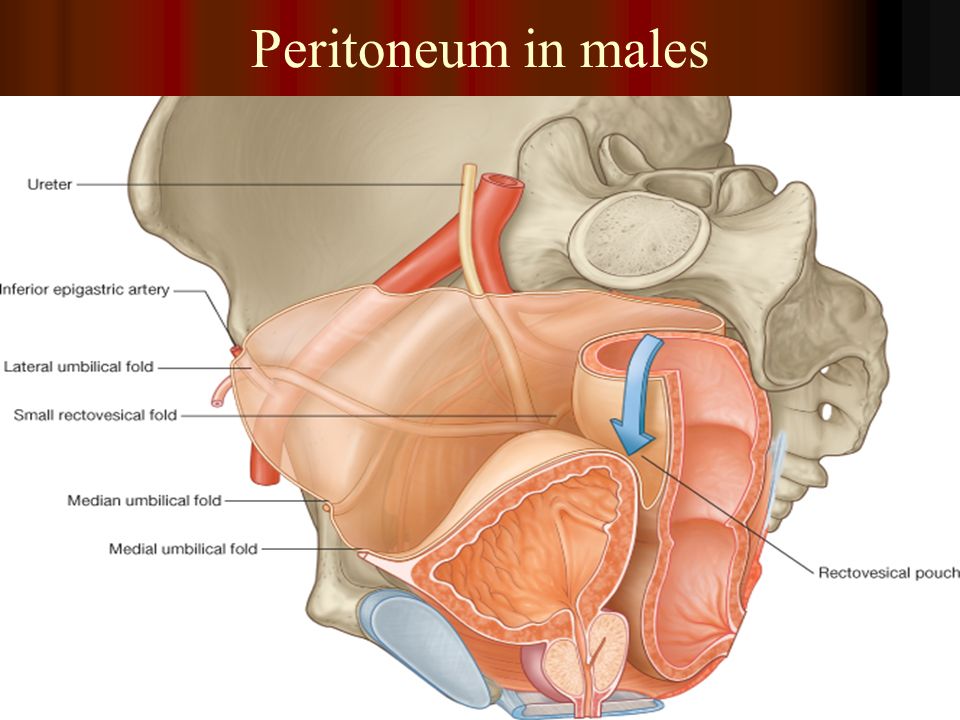
What do you prefer to learn with?
Videos Quizzes Both
“I would honestly say that Kenhub cut my study time in half.” – Read more. Kim Bengochea, Regis University, Denver
© Unless stated otherwise, all content, including illustrations are exclusive property of Kenhub GmbH, and are protected by German and international copyright laws. All rights reserved.Pelvis / Female Anatomy
Pelvis
The small pelvis is the lower half of the pelvis of a woman, in which the uterus with appendages, the bladder and rectum, blood vessels and nerves are located. The organs of the small pelvis are fixed to the walls of the pelvis with the help of ligaments and fascia. For ease of understanding, this design can be compared to a suspension bridge.
Front and back - bridge supports (pubis and sacrum). A bridge (vagina) is stretched between them. Ropes (bundles) stretch from the upper part of the supports to the bridge. From the back support (sacrum) - sacro-uterine ligaments.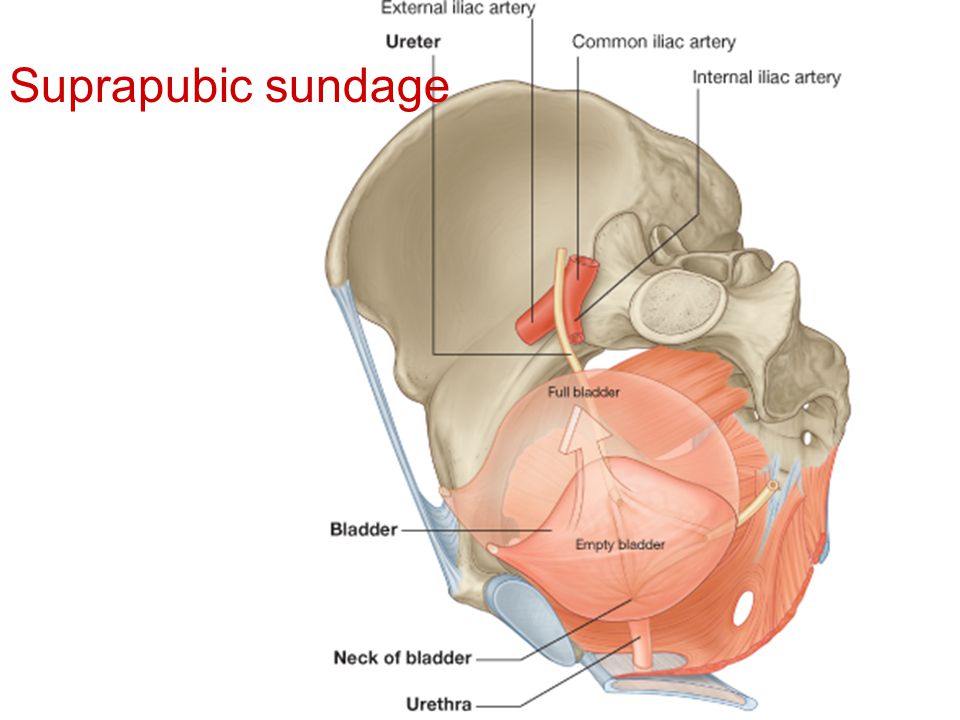 From the anterior support (pubis) - pubo-urethral ligaments.
From the anterior support (pubis) - pubo-urethral ligaments.
The bridge (vagina) can be compared to the membrane of a trampoline, and the ligaments of the pelvis to its springs.
The bladder lies on the anterior wall of the vagina like in a hammock.
The main pelvic fascia is the pubocervical fascia. This is a connective tissue sheet between the anterior wall of the vagina and the bladder. This fascia is the hammock, trampoline, or suspension bridge. She fascia is stretched from front to back with the help of the described ligaments, and on the sides is attached to the walls of the pelvis.
Defects in the ligamentous and/or fascial structures that occur during childbirth lead to various types of prolapse of the pelvic organs.
The most important supporting ligament is the sacro-uterine, which fixes the entire structure from above. With its defect, the connection between the bridge and its rear support is lost. The pubocervical fascia, having lost support from above, breaks away from the walls of the pelvis.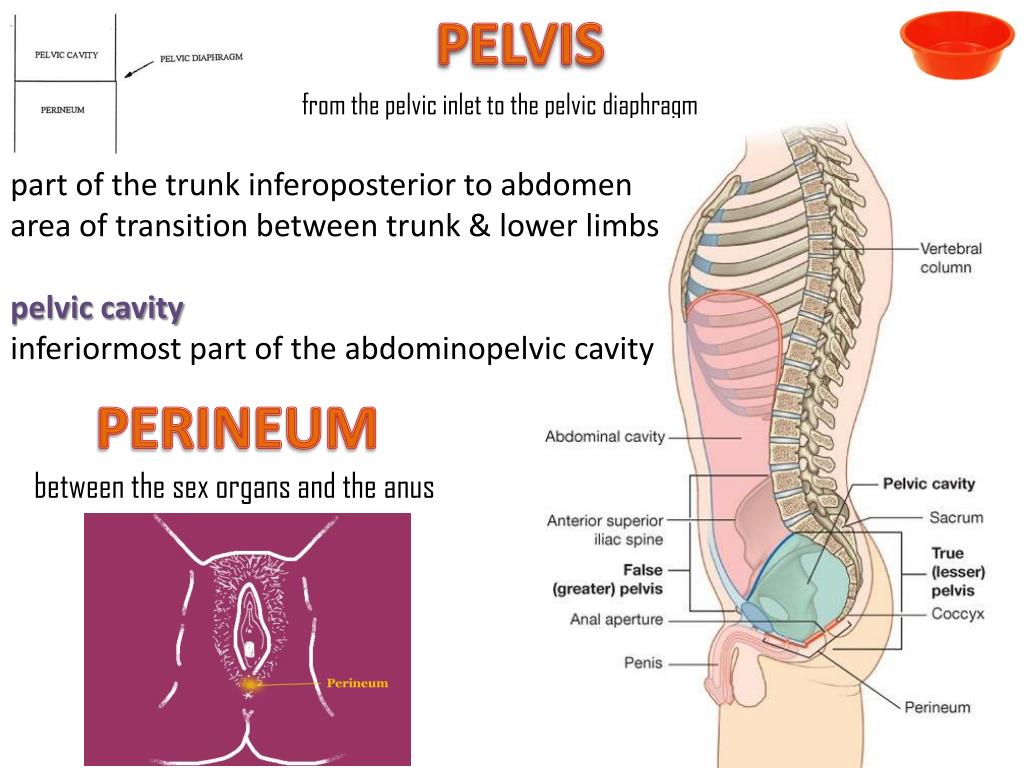 There is a prolapse of the uterus and the anterior wall of the vagina. Therefore, the most common type of prolapse (omission) is anteroapical (a combination of prolapse of the uterus and the anterior wall of the vagina).
There is a prolapse of the uterus and the anterior wall of the vagina. Therefore, the most common type of prolapse (omission) is anteroapical (a combination of prolapse of the uterus and the anterior wall of the vagina).
The pubo-urethral ligament plays an important role in the urinary continence mechanism. It fixes the urethra in the middle third, limits its mobility. A defect in this ligament causes abnormal mobility of the urethra and disrupts the mechanism of urinary retention.
Corresponding to this anatomical organ:
- Diseases
- Endometriosis
- Uterine prolapse
- Rectocele
- Operations
- Infiltrate resection
- Surgery for complications
- Enterocele correction
- Rectocele correction
- Correction of the entrance to the vagina
- Laparoscopic sacrovaginopexy
- OPUR
- Sacrospinal hysteropexy
Female Pelvis : Normal Anatomy
SUBSCRIBE
SUBSCRIBE
ANATOMICS
- Fallopian tube ampulla
- Fallopian tube funnel
- Bubble bottom
- Round ligament of uterus (Hunter)
- Round ligament of uterus (Hunter)
- Uterus
- Fallopian tube
- Cape
- External iliac artery
- Paravesical fossa
- Isthmus of uterus
- Isthmus of fallopian tube
- Suspension ligament of ovary
- Suspension ligament of ovary
- Transverse vesicle fold
- Right medial umbilical fold
- Right external iliac artery
- Right ureter
- Rectum
- Rectouterine ligament (Petit)
- Recto-uterine recess (Douglas)
- Vesicouterine cavity
- Sigmoid colon
- Ovarian ligament proper
- left ovary
Quick access Schematic drawings
Figure 1 - Surgical anatomy of the female pelvis (laparoscopy)
Figure 2 - Female pelvis: Uterus, Ovary, Recto-uterine cavity
No content available
DOWNLOAD APP
IMAIOS and certain third parties use cookies or similar technologies, in particular for audience measurement.