Cystic fibrosis test when pregnant
Cystic Fibrosis: Prenatal Screening and Diagnosis
Amniocentesis: A procedure in which amniotic fluid and cells are taken from the uterus for testing. The procedure uses a needle to withdraw fluid and cells from the sac that holds the fetus.
Amniotic Fluid: Fluid in the sac that holds the fetus.
Carrier: A person who shows no signs of a disorder but could pass the gene to their children.
Carrier Screening: A test done on a person without signs or symptoms to find out whether he or she carries a gene for a genetic disorder.
Chorionic Villus Sampling (CVS): A procedure in which a small sample of cells is taken from the placenta and tested.
Cystic Fibrosis (CF): An inherited disorder that causes problems with breathing and digestion.
Diagnostic Test: A test that looks for a disease or cause of a disease.
Embryo: The stage of development that starts at fertilization (joining of an egg and sperm) and lasts up to 8 weeks.
Ethnic-Based Screening: Screening recommended for people who belong to an ethnic group or race that has a high rate of carriers of a specific genetic disorder.
Expanded Carrier Screening: A blood test to screen for a large number of genetic disorders.
Fetus: The stage of human development beyond 8 completed weeks after fertilization.
Gene: A segment of DNA that contains instructions for the development of a person’s physical traits and control of the processes in the body. The gene is the basic unit of heredity and can be passed from parent to child.
Genetic Counselor: A health care professional with special training in genetics who can provide expert advice about genetic disorders and prenatal testing.
Genetic Disorder: A disorder caused by a change in genes or chromosomes.
In Vitro Fertilization (IVF): A procedure in which an egg is removed from a woman’s ovary, fertilized in a laboratory with the man’s sperm, and then transferred to the woman’s uterus to achieve a pregnancy.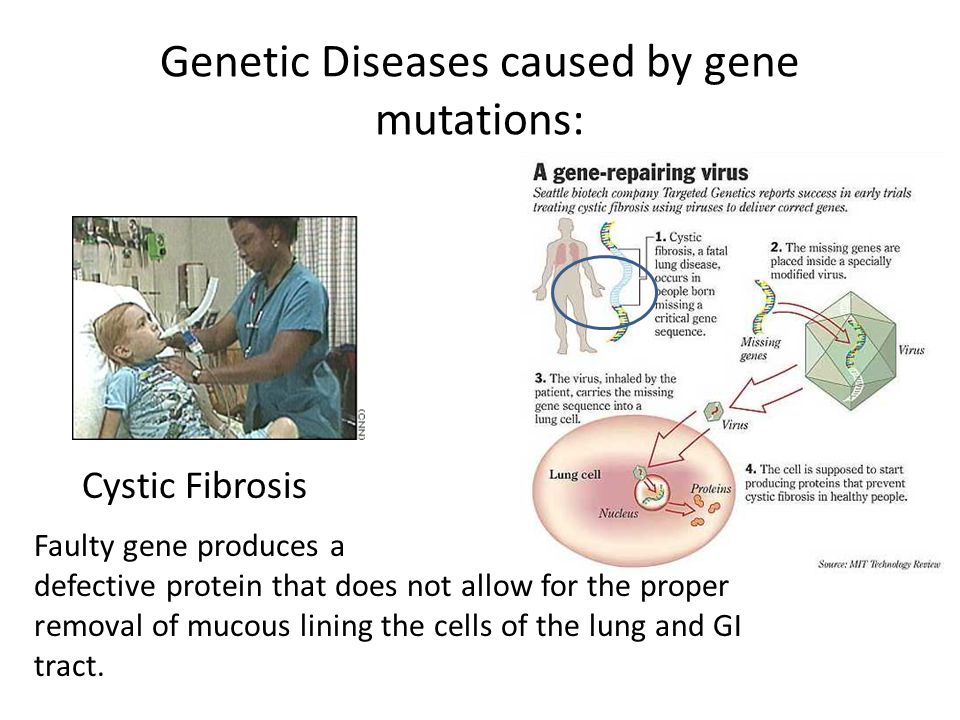
Mutation: A change in a gene that can be passed from parent to child.
Obstetric Care Provider: A health care professional who cares for a woman during pregnancy, labor, and delivery. These professionals include obstetrician– gynecologists (ob-gyns), certified nurse–midwives (CNMs), maternal–fetal medicine specialists (MFMs), and family practice doctors with experience in maternal care.
Obstetrician–Gynecologist (Ob-Gyn): A doctor with special training and education in women’s health.
Placenta: An organ that provides nutrients to and takes waste away from the fetus.
Preimplantation Genetic Testing: A type of genetic testing that can be done during in vitro fertilization. Tests are done on the fertilized egg before it is transferred to the uterus.
Sperm: A cell made in the male testicles that can fertilize a female egg.
Cystic Fibrosis Prenatal Screening and Diagnosis
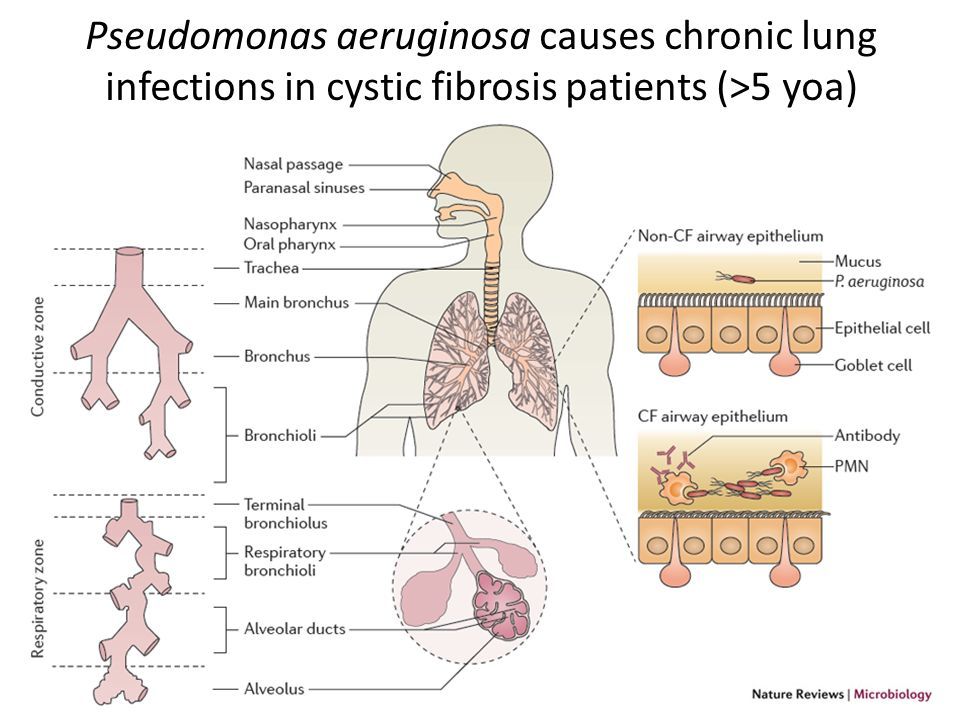
Cystic fibrosis (CF) is a genetic disorder.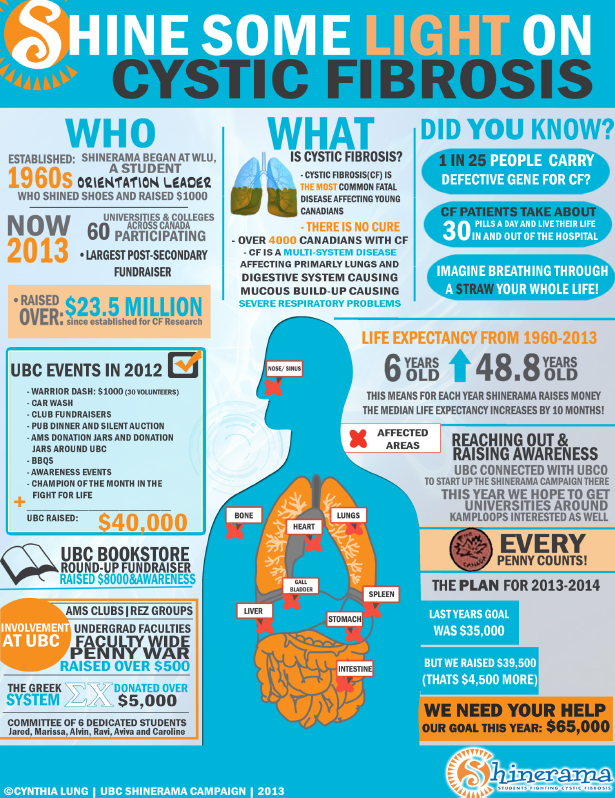 It causes thick mucus to collect in your lungs and intestines. This causes problems with breathing and digestion. The damage is permanent. CF gets worse over time. People who have CF have a shorter life expectancy. However, thanks to modern medicine, people who have CF are living longer, healthier lives than ever before.
It causes thick mucus to collect in your lungs and intestines. This causes problems with breathing and digestion. The damage is permanent. CF gets worse over time. People who have CF have a shorter life expectancy. However, thanks to modern medicine, people who have CF are living longer, healthier lives than ever before.
Two parents who have the CF gene can pass it on to their baby. Children have a 25% chance of having CF if both parents have one copy of the gene. Your doctor may perform a prenatal screening to test for CF if both parents know they carry the gene. This is performed while you are pregnant. It checks for any health problems with your baby before they are born. The screening also can detect other genetic disorders. This includes birth defects, and neural tube defects.
Path to improved well being
At your first prenatal visit, your doctor will talk to you about screening and tests. Although they may offer suggestions, it is your choice to do the screenings or not.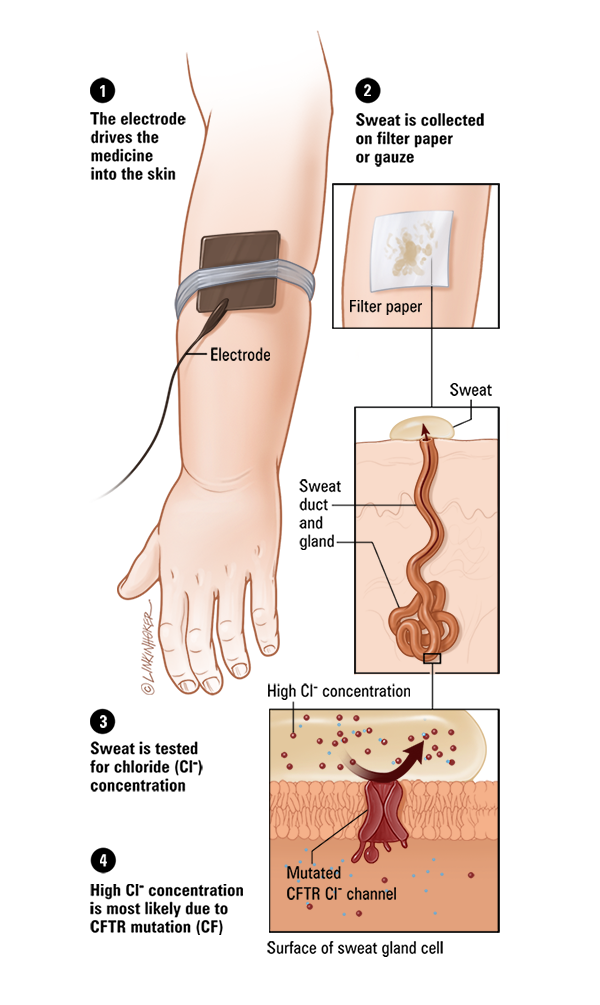
If you don’t know if you have or carry CF and would like to find out, you may choose to do carrier screening test first. This is a simple method to test you or your partner for the CF gene.
Your doctor will collect a blood, saliva, or tissue sample from inside your cheek. Carrier screening is done one person at a time. It can be done before or during pregnancy. The possible results are:
- You (or your partner) test negative as a carrier. The other person does not need to be tested.
- You (or your partner) test positive as a carrier. The other person should be tested.
- You and your partner both test positive as carriers. If you are pregnant, you should consider the prenatal testing to see if your baby has CF. If you are not pregnant but are trying, talk to your doctor about your options. You may consider adopting or using fertility treatment to avoid the CF gene.
Screening for CF in a baby can be done one of two ways.
- Chorionic villus sampling (CVS). Your doctor collects a sample of tissue from your placenta. This test is done between 10 and 13 weeks of pregnancy.
- Your doctor collects a sample from your amniotic fluid. This test is done between 15 and 20 weeks of pregnancy.
If the prenatal screening is positive for CF, you have two options.
- You can continue with your pregnancy. The diagnosis does not affect ongoing prenatal care. In the remaining months, do research to learn more about CF. Talk to your doctor about treatment options. You may consider joining a support group.
- You can end your pregnancy. This decision consists of legal and moral considerations.
At your first prenatal visit, your doctor will talk to you about screening and tests. Although they may offer suggestions, it is your choice if you want to do the screenings or not.
Things to consider
Although screening can be helpful, it also can create added worry or concern.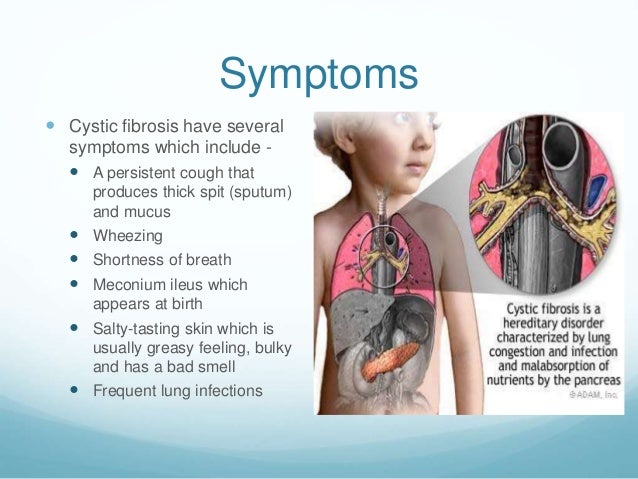 If you choose not to screen during pregnancy, most states check for CF during newborn screening. This is a series of tests your baby undergoes in the hospital after birth. These include blood, hearing, and heart tests. Talk to your doctor to see what your state’s testing includes.
If you choose not to screen during pregnancy, most states check for CF during newborn screening. This is a series of tests your baby undergoes in the hospital after birth. These include blood, hearing, and heart tests. Talk to your doctor to see what your state’s testing includes.
Keep in mind that no screening is 100% effective. Carrier and prenatal screenings cannot check for all gene mutations. If the tests are negative, there still is a rare chance you carry CF or your baby could have CF. Talk to your doctor if:
- You and your partner both have CF.
- You and your partner are known carriers for CF.
- You and your partner have a family history of CF.
- You and your partner are pregnant or trying to become pregnant and want to learn more about genetic testing.
Questions to ask your doctor
- What are the risks and benefits of CF prenatal screening?
- Does my state test for CF during the newborn baby screening?
- If my partner or I test negative in the carrier screening, what is the chance our baby could still have CF?
- If we have a child with CF, what are the chances our other children will have CF?
- Are there other prenatal screening tests that I should consider?
Resources
American College of Obstetricians and Gynecologists: Cystic Fibrosis: Prenatal Screening
March of Dimes: Cystic Fibrosis and Pregnancy
National Institutes of Health, MedlinePlus: Cystic Fibrosis
Copyright © American Academy of Family Physicians
This information provides a general overview and may not apply to everyone.![]() Talk to your family doctor to find out if this information applies to you and to get more information on this subject.
Talk to your family doctor to find out if this information applies to you and to get more information on this subject.
Diagnosis of cystic fibrosis during pregnancy
Recently, the world began to carry out genetic tests to determine cystic fibrosis in infants. A blood test is taken from the child, if it turns out that the level of immunoreactive trypsin is at high levels, the newborn is at risk. But, to confirm the disease or its absence, an additional study of salts in the sweat fluid is carried out. Some parents ask: why is it necessary to undergo a study with a confirmed disease? To answer this question, it is necessary to consider this disease in more detail and find out what it can lead to.
Cystic fibrosis is a severe genetic disease caused by a mutation of the CFTR gene on the seventh chromosome, which cannot be cured. The mutation leads to the fact that the protein that regulates the movement of electrolytes through the cell structure is produced in small quantities or ceases to be produced at all.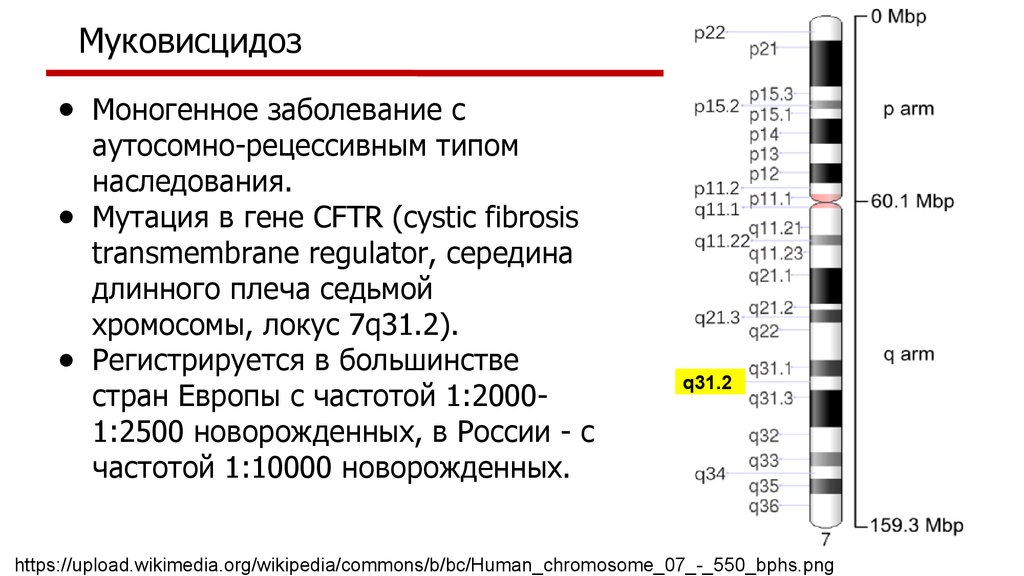
As a result of impaired function of the synthesized protein, the mucus produced by the respiratory organs, as well as the gastrointestinal tract, becomes viscous, thick, which leads to damage to these organs and sclerotic changes develop in them. It is impossible to get infected with cystic fibrosis, since people are already born with this disease, and the disease affects both girls and boys with the same frequency.
Patients often get sick with bronchitis, pneumonia, cirrhosis of the liver or cholelithiasis caused by bile stasis can also develop.
Common manifestations (symptoms of the disease) include:
- chronic wet cough;
- audible rales in the lungs;
- recurring illnesses like SARS, pneumonia and bronchitis;
- weakness and lethargy.
People who have only one defective gene are called carriers. In a child, during examination, this disease can be detected only if the parents are carriers of mutations.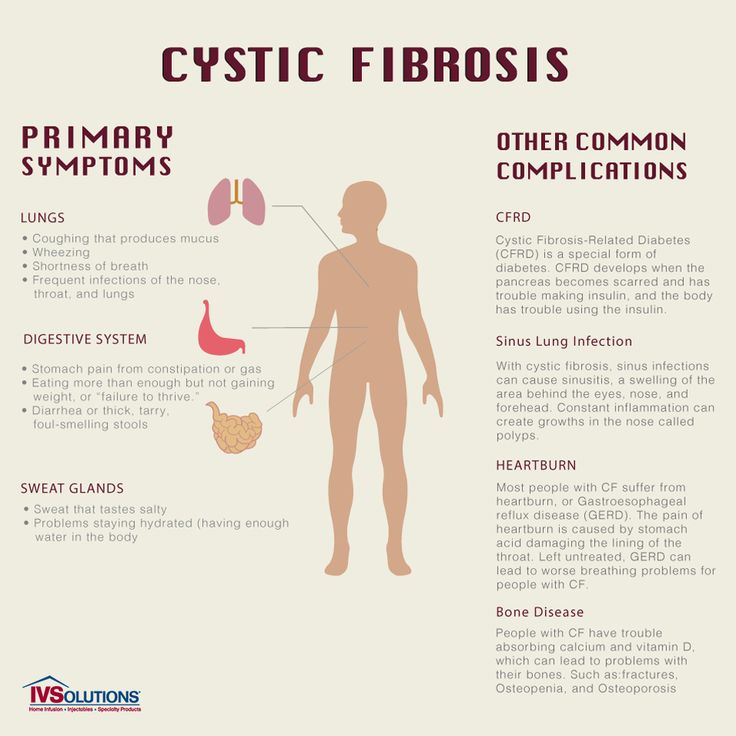
Non-invasive prenatal DNA testing and early detection of cystic fibrosis
Carriers of the defective gene have a 25% increased risk of having a child diagnosed with cystic fibrosis with each subsequent pregnancy. To prevent this from happening, it is necessary to identify which defect in the CFTR gene provoked the disease in the child.
The easiest and cheapest way is to be tested for various types of mutation, of which there are about thirty. If the test reveals a single defect, the entire gene sequence will need to be analyzed by sequencing. This test allows you to identify all existing mutations.
This must be done in order to know which type of mutations the parents are and, if necessary, during pregnancy or in vitro fertilization, examine the fetus for their presence. There are several methods for diagnosing monogenic diseases, including cystic fibrosis:
— Before pregnancy, women are advised to do preimplantation genetic diagnosis in the IVF cycle (PGD).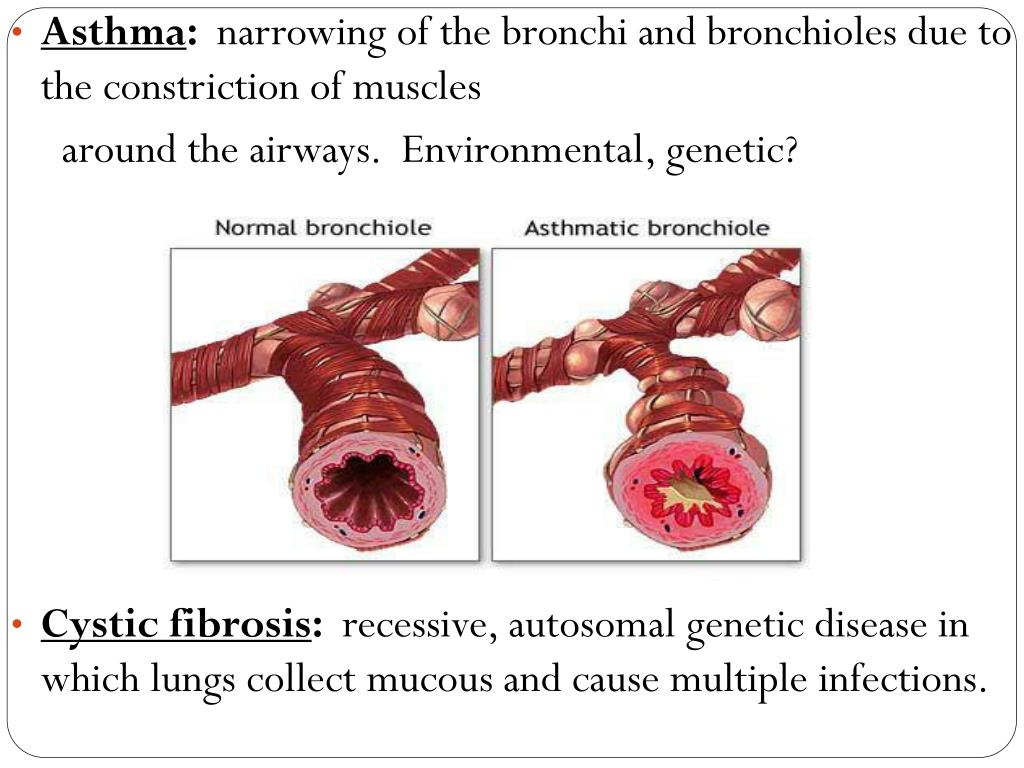
Before transferring an embryo into the uterine cavity, some of its cells are examined for the presence of genetic diseases. After the diagnosis, a conclusion is issued on the suitability of the transfer of the examined embryo.
- During pregnancy. In case of serious abnormalities in the fetus due to chromosomal abnormalities, at the tenth to twelfth week of pregnancy, the placenta is taken by puncture of the anterior abdominal cavity.
Further, the material is checked for the carriage of gene mutations, if they are not detected or one mutation is detected, you can not be afraid that the child will be born sick. In a situation where two defective genes are identified, the diagnosis is considered confirmed, and parents are faced with the choice of having a child with cystic fibrosis or terminating the pregnancy.
- During pregnancy, safe option. There is also a safe and absolutely non-traumatic method for studying the genetic health of the unborn child during pregnancy - a non-invasive prenatal test.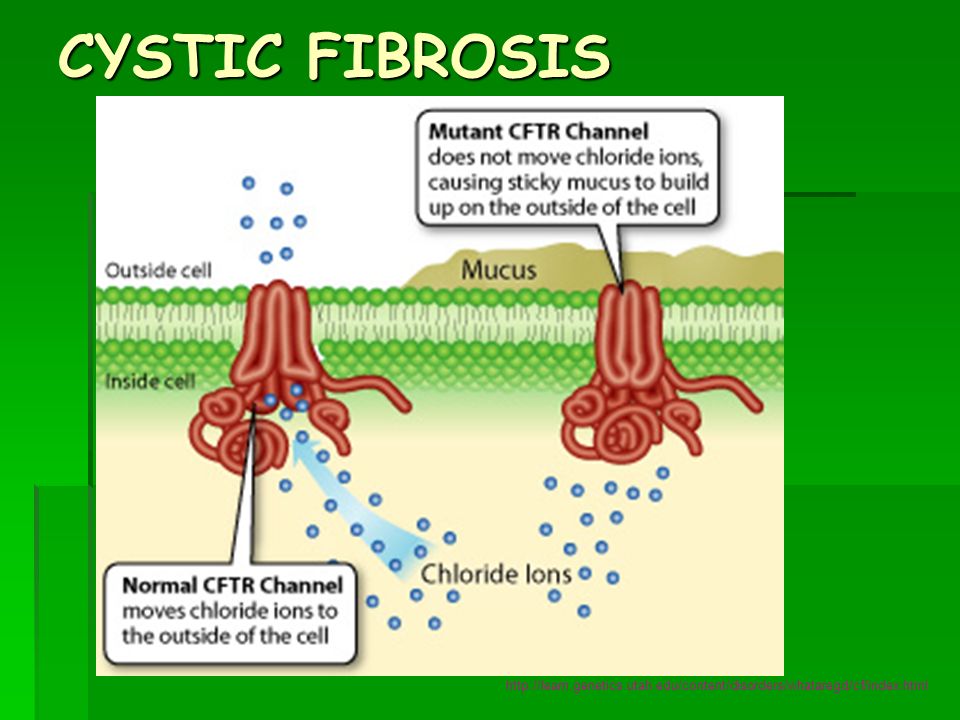
In Russia, only one European test examines fetal DNA for 100 monogenic diseases, this is the VERAgene test, manufactured in Cyprus.
The test is carried out as early as 10 weeks of gestation and only maternal venous blood is required for the test. The accuracy of the study is the same as with invasive procedures.
We sincerely hope that over time new drugs will appear that can regulate the work of genes, and the prescription of the drug will depend on what type of gene mutation the child has.
To take the VERAgene test, contact the Medical Genomics laboratory. Also, in case of a positive result, there will be an opportunity to consult with a practicing geneticist of our medical center for free.
When and why are genetic tests needed if a child has cystic fibrosis?| Center for Genetics and Reproductive Medicine Genetico
November 21, 2016
In many countries, all newborns are now screened for cystic fibrosis. If an elevated level of immunoreactive trypsin is detected in the blood of a child, he is referred to the risk group, and the final diagnosis is established (or excluded) based on the study of salts (chlorides) in sweat fluid. Many parents may have a natural question: why undergo a genetic test if the child's diagnosis has already been confirmed? Let's figure it out.
Many parents may have a natural question: why undergo a genetic test if the child's diagnosis has already been confirmed? Let's figure it out.
Cystic fibrosis is a hereditary disease. And it is associated with a malfunction of the CFTR gene on chromosome 7. This gene produces a special protein in all healthy people, which is necessary to maintain the low viscosity of the mucus produced by various hollow organs (mainly in the respiratory and digestive systems). If a given gene carries a mutation (breakdown/defect) on both 7th chromosomes (received from both mother and father), its protein is not produced or produced in very small quantities. If the mutation is present only on one of the 7 chromosomes, this does not manifest itself in any way and is called “carriage”. Thus, if your child is diagnosed with cystic fibrosis, you and your spouse both carry mutations in the CFTR gene.
This means that with each subsequent pregnancy you have a high risk that the baby will also be sick with cystic fibrosis.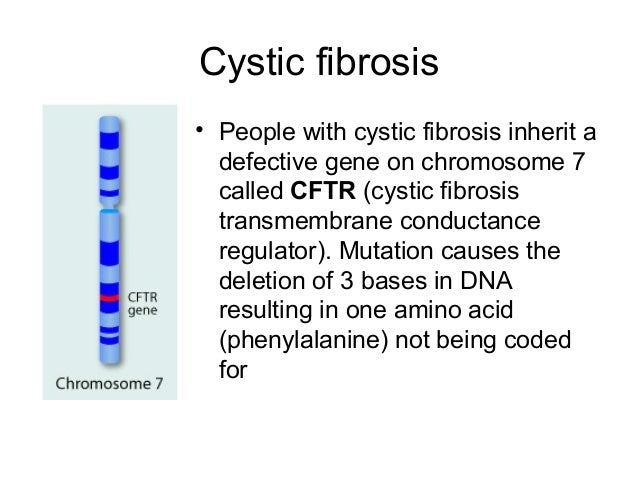 This risk is 25%.
This risk is 25%.
If you want to protect yourself from having a child with cystic fibrosis again, you must first find out which mutations (defects) in the CFTR gene caused the disease in your child. The simplest and least expensive test is a test for mutations that occur most often. There are about 30 of them, and all can be tested at the same time. If, however, no mutations are detected, or only one is detected, the entire gene sequence will have to be tested to search for rarer ones. This test is called sequencing. It will identify all mutations that may not have been previously described in any patient with cystic fibrosis in the world.
When you know which mutations you and your husband are carriers of, you can test them on the fetus (in the presence of pregnancy) or the embryo (in the event of conception with the help of IVF).
Now the most common prenatal diagnosis is when during pregnancy at a period of 10-12 weeks the fetal material (placenta) is taken through a puncture of the anterior abdominal wall. The resulting material is examined for the carriage of already known mutations. If no mutations are found, or only one mutation is found, the child will be healthy. If 2 mutations are found, then the diagnosis of cystic fibrosis can be considered established and the family faces a difficult decision to keep the pregnancy in order to give birth to a child with a hereditary disease, or to interrupt.
The resulting material is examined for the carriage of already known mutations. If no mutations are found, or only one mutation is found, the child will be healthy. If 2 mutations are found, then the diagnosis of cystic fibrosis can be considered established and the family faces a difficult decision to keep the pregnancy in order to give birth to a child with a hereditary disease, or to interrupt.
Preimplantation genetic diagnosis (PGD) is a better option for prenatal diagnosis. PGD allows you to examine the genetic status of an embryo obtained through in vitro fertilization (IVF) before it enters the uterine cavity and pregnancy occurs. In this case, you will not face the moral problem of terminating a pregnancy and at the same time you will know for sure that your unborn child will not suffer from cystic fibrosis.
In addition, in the near future, drug gene preparations will become available, the effect of which will depend on the type of mutation. Then the knowledge of which mutation your child has will be decisive in prescribing a particular drug.